The essential takeaway: Migraine isn’t a severe headache—it’s a genetic neurological disease causing intense pain affecting 1 in 5 women and 1 in 16 men. Linked to brain chemistry (like CGRP) and hormones, it disrupts daily life for over a billion people. New treatments targeting CGRP offer hope for reduced frequency and impact, emphasizing personalized care.
Ever dismissed a migraine as “just a headache”? Think again. Migraine is a debilitating neurological disease with a strong genetic component, impacting 1 in 5 women, 1 in 16 men, and over a billion globally. This article deciphers its four phases—from the subtle warning signs of the prodrome to the visual disturbances during the aura phase, the pulsing pain that disrupts daily activities, and the draining postdrome hangover. It explains WHO’s classification as a primary headache disorder, debunks myths about triggers like hormonal shifts or sensory stimuli, and reveals why this condition—far more complex than ordinary head pain—demands understanding beyond clichés.
- More than just a headache: defining what a migraine is
- The journey of an attack: understanding the four phases of migraine
- The science behind the pain: exploring the causes of migraine
- Common triggers: what can set off a migraine attack?
- The many faces of migraine: an overview of the main types
- Getting a diagnosis: how do you know it’s a migraine?
- Beyond the pain: the impact of migraine on daily life and mental health
- Taking Control: Management Strategies And Finding Hope
More than just a headache: defining what a migraine is
What is a migraine, really?
A migraine is a neurological disease with genetic factors affecting over a billion people globally. Classified by the WHO as a primary headache disorder, it causes intense, throbbing pain lasting 4–72 hours. Unlike common headaches, it disrupts daily activities completely, often requiring rest in dark, quiet spaces. Some people experience early warning signs like mood changes or food cravings (prodrome) before the pain starts.
Beyond head pain, migraines include nausea, vomiting, and sensitivity to light, sound, and smell. Visual disturbances like flashing lights or blind spots (aura) appear in some cases. These symptoms reflect neurological dysfunction, not just localized pain. According to WHO, migraines rank as the second leading cause of disability worldwide, surpassing diabetes and asthma in disability years.
A common but misunderstood condition
Migraines impact one in five women and one in sixteen men, with over a billion people worldwide affected. Genetic factors play a big role: 80-90% of migraineurs have family members with the condition. Women experience migraines three times more common in women due to hormonal fluctuations. Many notice links to menstrual cycles, pregnancy, or menopause. Despite its prevalence, migraines remain misunderstood, often dismissed as “bad headaches,” ignoring systemic effects like fatigue, mood shifts, and sensory overload.
Migraine vs. tension headache: key differences
Many confuse migraines with tension headaches. While both cause head pain, they differ significantly. Migraines often include nausea, vomiting, and sensitivity to light, with pain worsening during physical activity. Tension headaches rarely have these symptoms. Tension headaches typically affect both sides of the head and rarely cause sensitivity to light or sound.
| Feature | Migraine | Tension Headache |
|---|---|---|
| Pain quality | Throbbing or pulsing | Dull, tightening, pressure |
| Pain location | Often one-sided (unilateral) | Both sides of the head (bilateral) |
| Pain intensity | Moderate to severe | Mild to moderate |
| Associated symptoms | Nausea, vomiting, sensitivity to light and sound | Usually none; maybe mild sensitivity |
| Impact on activity | Worsened by physical activity, often debilitating | Does not typically prevent daily activities |
This table highlights critical distinctions. Migraines bring more intense pain and additional symptoms. They severely impact daily life, unlike tension headaches which are usually manageable. Mislabeling migraines risks ineffective treatment. For example, while 70% of tension headache sufferers work through pain, only 36% of migraineurs report the same, showing how much more disabling migraines are.
The journey of an attack: understanding the four phases of migraine
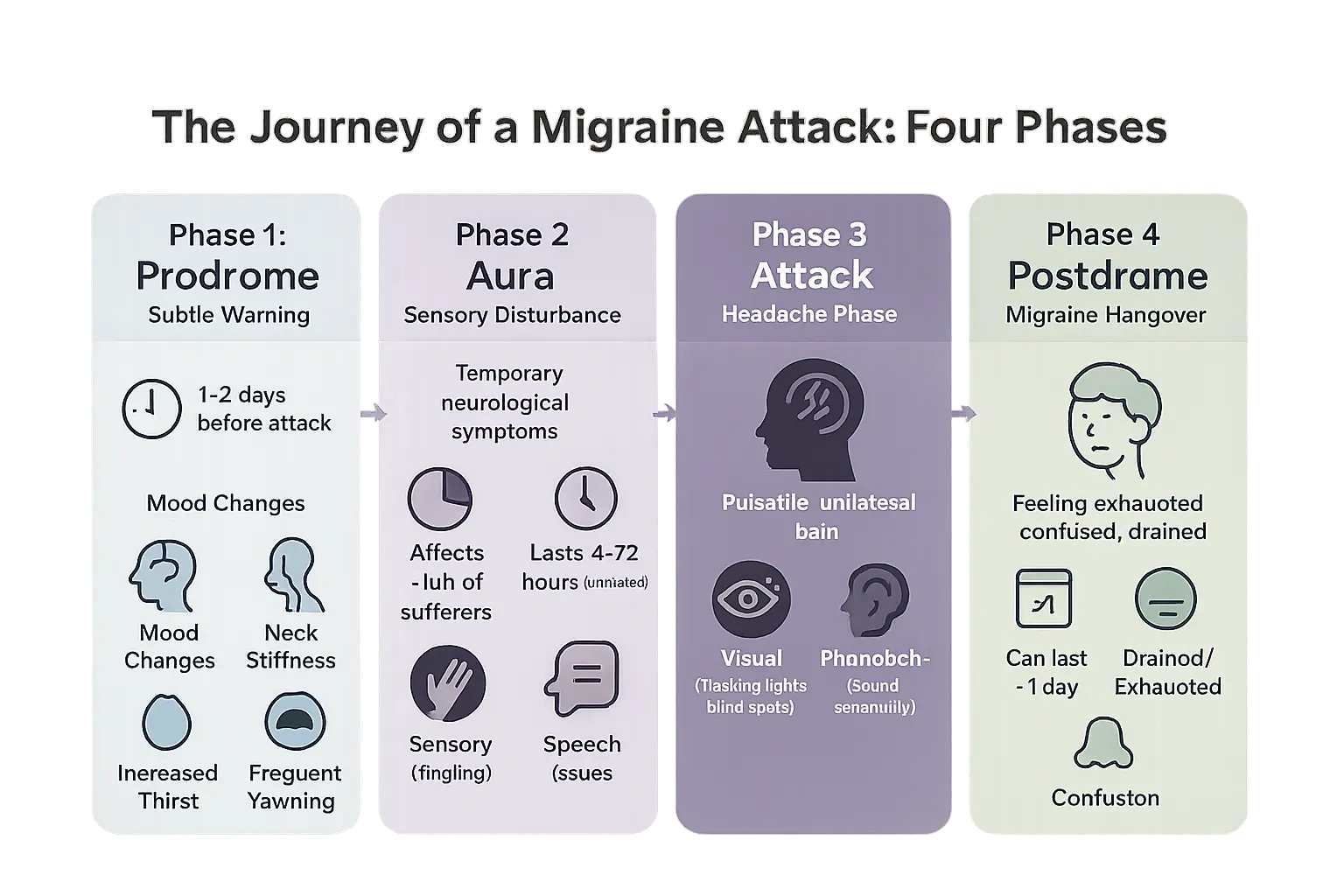
Phase 1: the prodrome (the subtle warning)
Before a migraine hits, your body might send early signals. This pre-attack phase, called prodrome, gives you a chance to prepare. Around 30-40% of migraine sufferers experience these warning signs up to 24 hours before pain begins. Symptoms like neck stiffness or food cravings often go unnoticed as migraine indicators. These subtle changes reflect underlying neurological shifts in brain chemistry, including CGRP fluctuations and dopamine variations.
- Mood changes (from depression to euphoria) – linked to serotonin level shifts
- Food cravings – often for salty or sweet foods
- Neck stiffness – early muscle tension response
- Increased thirst and urination – tied to hypothalamic activation
- Frequent yawning – associated with dopamine release patterns
Recognizing these early signs helps you take preventive action. Tracking symptoms improves attack prediction by 60%. This phase proves migraines aren’t sudden events – your brain starts changing days beforehand. Keeping a migraine journal with apps like Migraine Buddy helps identify personal patterns. For more details about these symptoms, check the full sequence of migraine symptoms.
Phase 2: the aura (the sensory disturbance)
Only 25-30% of migraineurs experience this neurological light show. The aura phase features temporary disturbances over 5-60 minutes. Visual symptoms dominate – think flashing lights, geometric shapes, or blind spots. Some get tingles or speech difficulties. The International Headache Society confirms these symptoms are fully reversible. Research shows women report auras more frequently than men, though prevalence varies globally – 31% in US studies vs 10-12% in Asian populations.
Visual disturbances never cause permanent damage despite their intensity. Some describe “silent auras” without subsequent headache, proving migraine’s complexity. Common visual patterns include scintillating scotoma (zig-zag patterns) and fortification spectra (castle wall shapes). Sensory auras might cause hand numbness or speech slurring that resolves before pain starts.
Phase 3: the attack (the headache phase)
This is the phase everyone recognizes. The pain builds over hours, described as throbbing and often one-sided. Physical activity worsens symptoms, turning simple tasks into challenges. Nausea strikes 70-90% of sufferers, with vomiting affecting 30%. Sensitivity impacts 85% (light), 80% (sound), and some smell sensitivity.
This phase lasts 4-72 hours untreated. The American Migraine Study II confirms 90% struggle to work during attacks. Pain location might shift as the attack progresses. The trigeminal nerve activation creates this pain, while cortical spreading depression explains symptom progression. This phase proves migraines disable through multiple sensory channels, not just head pain – light hurts, sounds overwhelm, and movement worsens symptoms.
Phase 4: the postdrome (the “migraine hangover”)
After the pain fades, 80% enter this “migraine hangover.” Imagine waking up after a storm – your brain feels foggy, tired, or emotionally drained. This phase lasts 24-48 hours with symptoms like:
- Exhaustion (more than regular tiredness)
- Confusion (similar to jet lag brain)
- Body aches (muscle tenderness)
- Difficulty concentrating (mental fatigue)
Sudden head movements might briefly bring back pain. Lingering activity changes explain why people feel “off” for days. The postdrome phase shows migraines affect your system long before and after the headache phase. Some experience “migraine hangover” without head pain, highlighting this condition’s complexity beyond pain perception. Brain imaging reveals persistent changes in blood flow and neural activity during this phase. 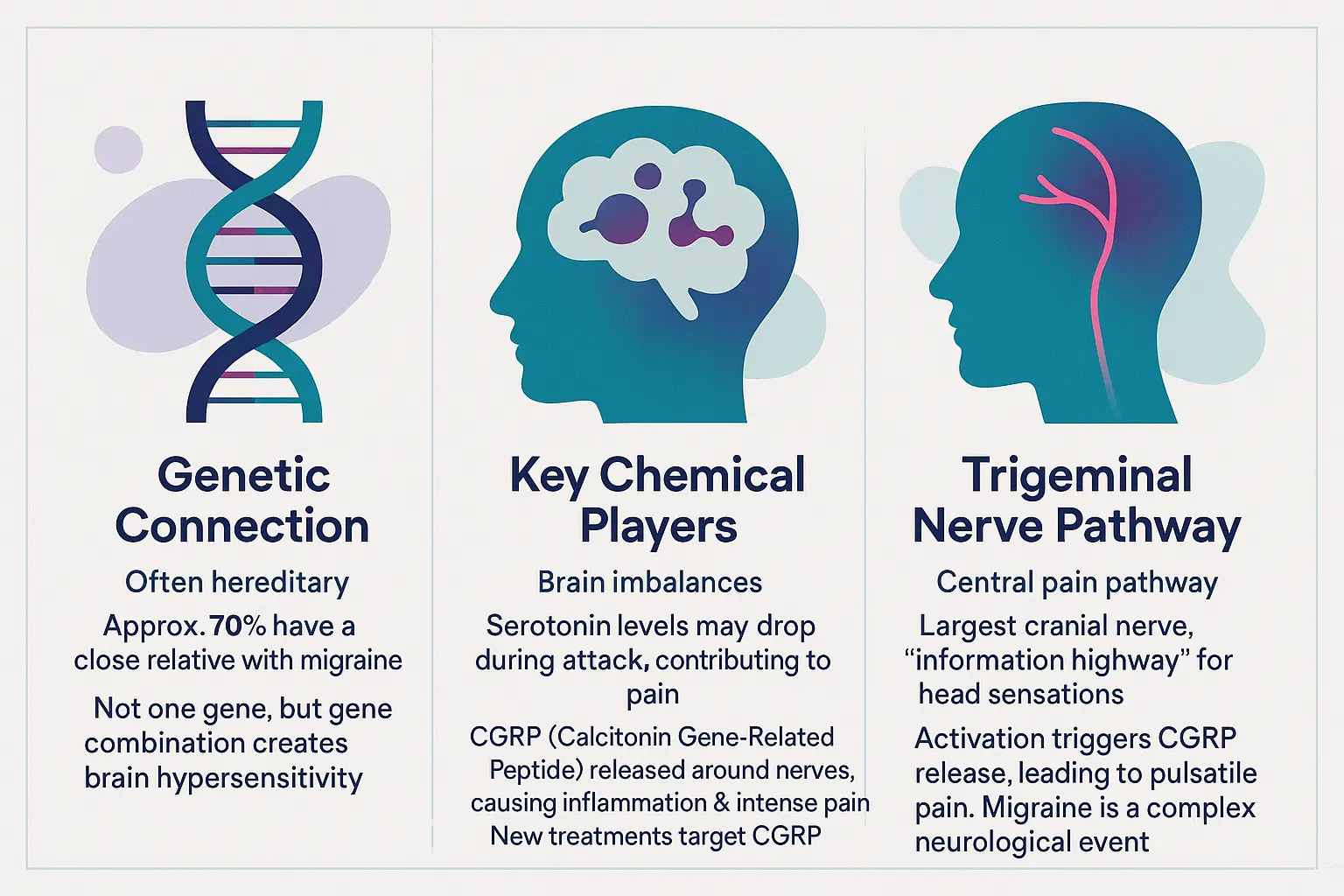
The science behind the pain: exploring the causes of migraine
Migraine isn’t just a bad headache. It’s a complex neurological disease involving genetic predispositions, chemical messengers, and overactive pain pathways. Let’s break down the science in simple terms about what really happens inside your head during a migraine attack.
The genetic connection: is migraine hereditary?
Did you know 70% of migraine sufferers have a close relative with the same condition? Harvard Health confirms this strong genetic component. It’s not about a single “migraine gene” but multiple genetic variations creating a sensitive brain environment.
Think of it like having a garden extra sensitive to weather changes. Some people inherit genetic “wiring” that makes their brain more reactive to triggers. This explains why migraines often run in families – it’s your brain’s sensitivity, not your family recipes, that gets passed down.
The brain in a state of alert: key chemical players
Two main chemicals drive migraine pain: serotonin and CGRP. You might know serotonin as the “happy chemical,” but during migraines, its levels drop dramatically (The role of serotonin). Think of it like a security system that suddenly stops working properly – leaving your brain’s pain sensors more reactive.
CGRP acts like a fire alarm protein. Normally helpful for blood pressure regulation, it becomes overactive during migraines, causing inflammation and intense pain. Modern treatments like monoclonal antibodies and gepants target this chemical specifically, acting as “CGRP blockers” that prevent pain signals.
The trigeminal nerve: a central pathway for pain
Meet your face’s emergency hotline – the trigeminal nerve. This is your brain’s main pain highway for head sensations. When activated, it releases CGRP like pouring gasoline on a fire, creating that throbbing pain.
This nerve doesn’t just carry pain signals – it creates them. CGRP causes blood vessels around the brain to dilate while activating nerve cells. This creates a feedback loop where pain signals get amplified, like a microphone too close to a speaker creating escalating sound – similar to migraines’ escalating pain pattern.
Contrary to old beliefs about blood vessels, migraines are neurological events. The trigeminal nerve acts as both sensor and signal booster, explaining why migraines feel so different from regular headaches. This discovery changed treatment approaches from blood vessel focus to targeted neurochemical interventions.
Connecting the dots: brain sensitization
Genetic predisposition creates a sensitive brain environment. When triggers activate, they set off the CGRP alarm through the trigeminal nerve highway. Meanwhile, serotonin’s drop removes your brain’s natural pain-dampening mechanisms.
This combination creates central sensitization – your brain’s pain volume gets turned up to maximum. Suddenly, normal stimuli like light, sound, or touch become painful. It’s not in your head; your brain processes sensations differently during attacks.
Understanding these mechanisms shows migraines aren’t “all in your head” – they’re about your brain’s complex responses. This knowledge opens doors to targeted treatments rather than just masking symptoms with general painkillers.
Common triggers: what can set off a migraine attack?
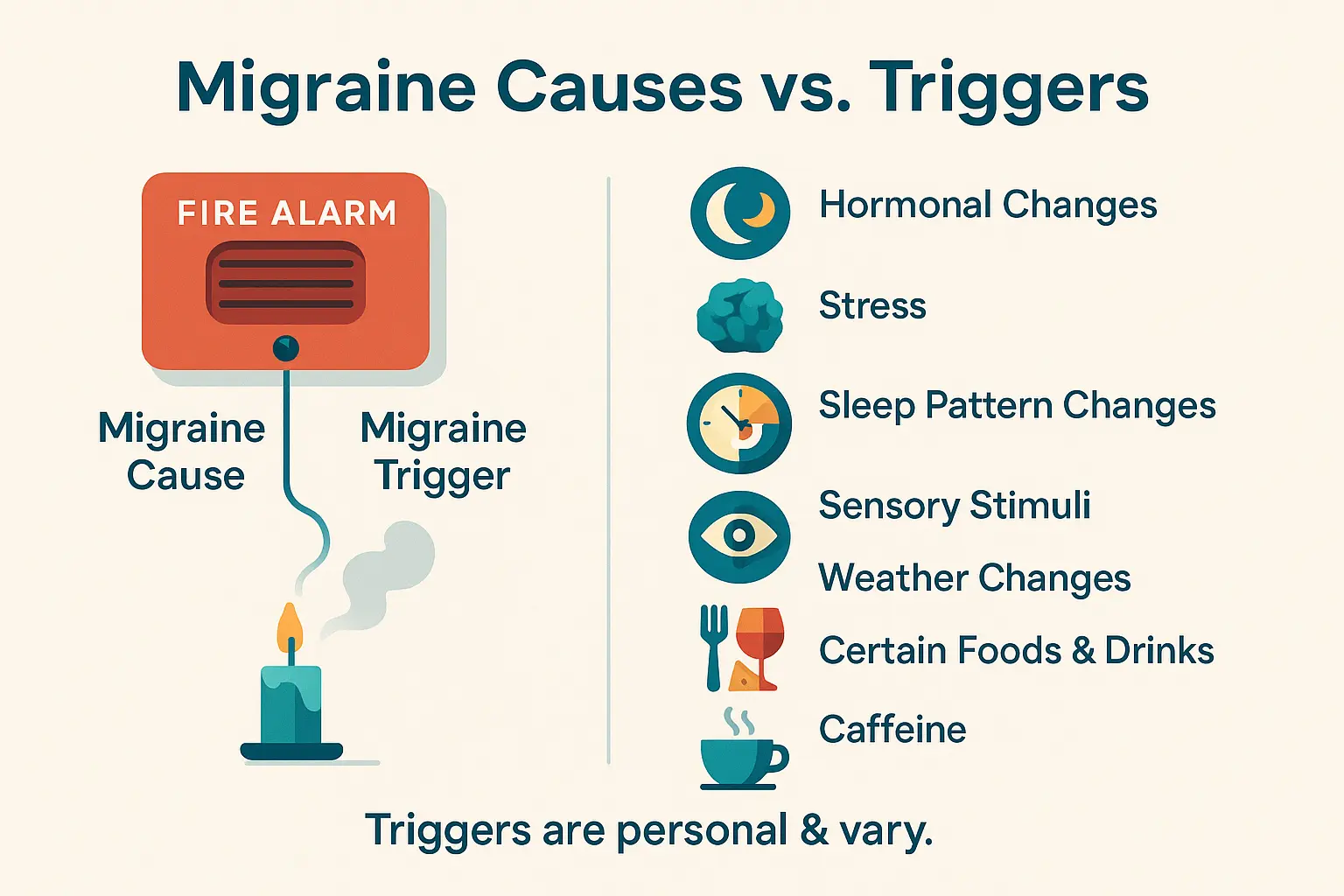
Distinguishing triggers from causes
Migraine is a neurological disease you’re born with, like a smoke alarm wired too sensitively in your brain. Understanding your specific migraine causes and triggers helps clarify this distinction. Causes relate to your genetic wiring and brain chemistry, while triggers are like smoke from a candle that sets off the alarm.
This isn’t about blame or lifestyle choices. Triggers activate your migraine-prone brain through hormonal shifts, weather changes, or even a glass of wine – but these aren’t “causing” migraines like faulty wiring causes electrical fires. Your sensitivity has a biological basis, not personal failing.
A list of potential culprits
While every migraine brain reacts differently, common triggers affect many sufferers:
- Hormonal changes in women – Estrogen fluctuations during menstrual cycles, pregnancy, or menopause dramatically increase risk through complex brain chemistry interactions
- Stress – Both chronic pressure and sudden relaxation (“let-down migraines”) disrupt brain’s chemical balance
- Sleep pattern changes – Even weekend lie-ins can destabilize your brain’s internal clock
- Sensory overload – Flickering lights, loud noises, and strong odors overstimulate migraine-prone nervous systems
- Weather changes – Barometric pressure shifts affect 53% of sufferers by altering brain fluid dynamics
- Food factors – Aged cheeses (tyramine), processed meats (nitrates), and red wine (histamine) create chemical imbalances
- Caffeine’s paradox – Too much excites the brain, but sudden withdrawal causes rebound effects
- Hydration issues – Missing meals or dehydration stresses your nervous system through blood sugar and electrolyte changes
Think of these as potential “bucket fillers” – when your metaphorical bucket gets full, migraines happen. What affects one person might not affect another. This variability explains why keeping a migraine journal is essential for personalized management.
Interestingly, some perceived triggers might be early symptoms. That chocolate craving before a migraine might be your brain’s prodrome phase, not the cause. Weather sensitivity relates to pressure changes affecting brain fluid balance, not just temperature shifts. Recognizing these nuances helps prevent unnecessary restrictions while focusing on true prevention strategies.
The many faces of migraine: an overview of the main types
Migraines aren’t just bad headaches. They’re complex neurological conditions with multiple faces. Understanding these variations helps patients and doctors create better treatment plans. Let’s explore the key types while keeping things clear and practical.
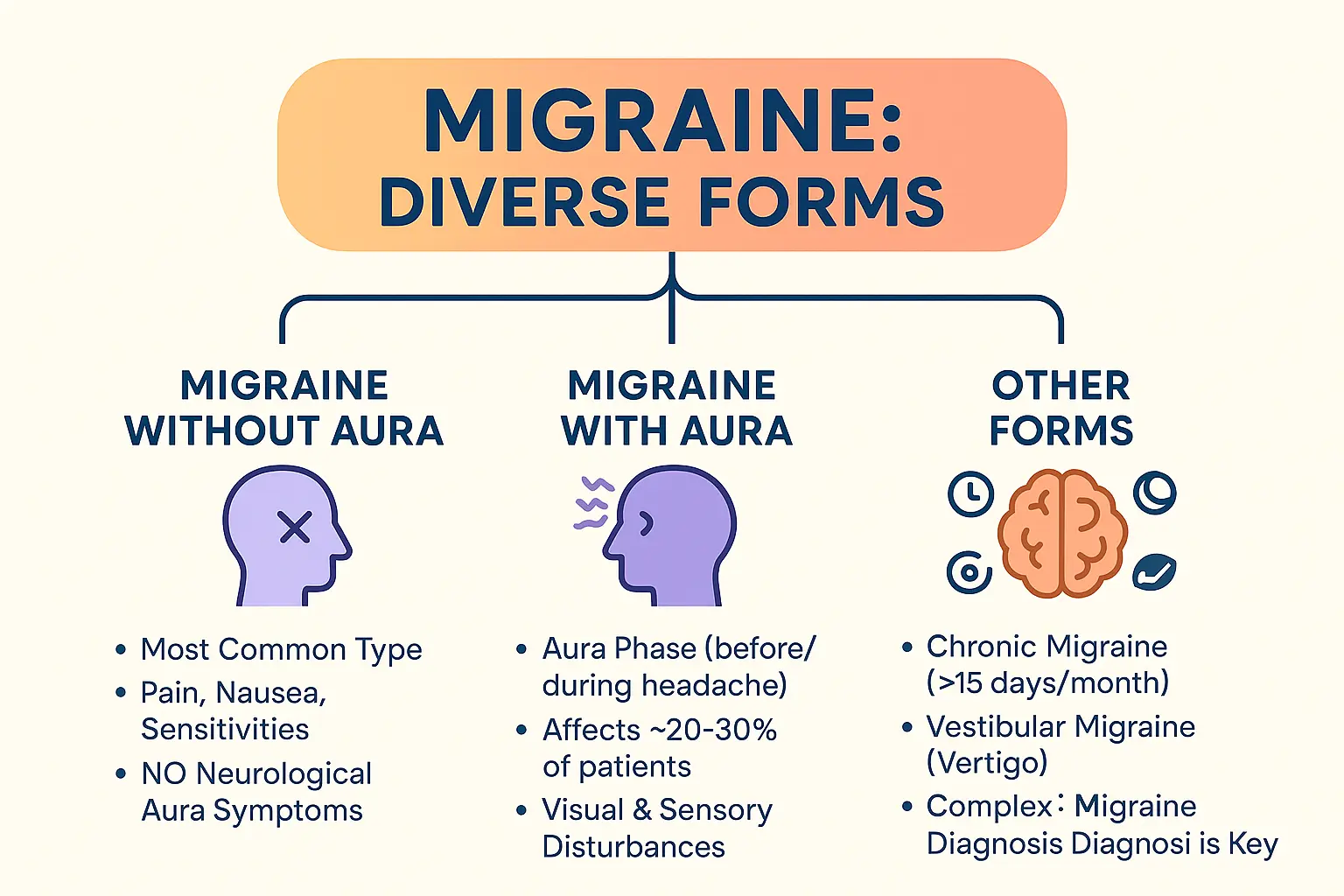
Migraine without aura
This is the most common form, affecting 70-75% of migraine sufferers. It features moderate to severe pulsating pain, usually on one side of the head. Common symptoms include nausea, sensitivity to light/sound, and worsened pain with physical activity.
Crises last 4-72 hours without treatment. Women experience this type more frequently, with hormonal changes acting as key triggers. Daily life often gets disrupted – imagine trying to work or care for family while battling these symptoms. Common triggers include stress, sleep changes, certain foods, and sensory stimuli like bright lights.
Migraine with aura
About 25-30% of migraine patients experience aura – temporary neurological disturbances before or during attacks. Visual disturbances are most common: flashing lights, blind spots, or zig-zag patterns. Some people get sensory symptoms like tingling or speech difficulties.
Aura symptoms develop slowly over 5-60 minutes. A 2020 Korean study found 29.4% of migraine patients had visual aura. While less common than migraine without aura, many people experience both types at different times. This variation shows how unpredictable migraines can be.
A word on other forms
Chronic migraine affects 2% of the population, with headaches occurring 15+ days monthly. It’s often linked to medication overuse, stress, and sleep issues. Vestibular migraine causes dizziness and vertigo, sometimes without head pain. Menstrual migraine impacts up to two-thirds of women, tied to hormonal fluctuations around periods.
These variations highlight why proper diagnosis matters. For more details about these less common forms, exploring the different types of migraines can provide valuable insights.
Getting a diagnosis: how do you know it’s a migraine?
Receiving a migraine diagnosis can feel uncertain. Unlike infections or fractures, there’s no single test to confirm it. Instead, doctors rely on your unique story to ensure accurate diagnosis. This process, though sometimes frustrating, helps avoid misdiagnosis while building a personalized treatment plan.
The role of your medical history
Migraine diagnosis relies on clinical evaluation, not scans. Doctors ask detailed questions about symptoms, frequency, and impact. Key criteria? At least five attacks meeting specific guidelines: headache lasting 4–72 hours untreated, one-sided pulsating pain, aggravation from routine activities, and nausea/light sensitivity. These four factors help differentiate migraines from other headaches, ensuring consistency in diagnosis.
Why there isn’t a “migraine test”
Modern medicine lacks blood tests or scans to “see” migraines. Brain imaging like MRI might be ordered to exclude serious causes – tumors, aneurysms, or infections – but these act as safety nets, not diagnostic tools. Studies show imaging detects critical issues in just 0.18% of typical cases. Your symptom timeline remains the clearest indicator, avoiding unnecessary radiation or costs from excessive testing.
The importance of a migraine diary
Tracking experiences transforms guesswork into data. A diary reveals patterns like triggers (weather shifts, specific foods), medication effectiveness, and early warning signs (e.g., visual aura or mood changes). Doctors use this information to personalize treatment. Apps or simple notebooks can capture these patterns, becoming your personal migraine fingerprint over time.
Diagnosis is like solving a puzzle – your symptoms are the pieces. When patterns emerge, doctors can finally say: “This is migraine.” Understanding your condition empowers better management, turning chaos into clarity through collaboration with healthcare providers.
Beyond the pain: the impact of migraine on daily life and mental health
The invisible burden
Migraine isn’t just head pain – it’s a life-altering condition. Imagine canceling family plans last-minute due to an attack. This affects millions: 82% face career setbacks, with 22% switching jobs. The unpredictability breeds constant anxiety: will today be a “good day” or one spent in darkness? Basic tasks become obstacles – 24% need help with chores, while 44% avoid driving during attacks.
Workplaces often misunderstand migraines. Though 89% report reduced work productivity, only 47% feel employer support. Social life suffers: 32% experience relationship strain, 41% abandon hobbies. These hidden struggles shape decisions daily. Family life changes too – 40% of parents reduce involvement in children’s activities, while 38% see intimacy with partners fade.
The link between migraine, anxiety, and depression
Migraine reshapes mental health. Research from Semantic Scholar (2025) shows 22% develop anxiety, 26% face depression – 5 times higher than average. Fear of attacks fuels anxiety, while chronic pain erodes resilience. 52% report disrupted sleep, creating a cycle where poor rest worsens symptoms.
Biological links exist: shared brain pathways involving serotonin mean treating one condition often helps the other. This explains why amitriptyline helps with both migraines and mood disorders. Cognitive behavioral therapy (CBT) also works by addressing psychological impacts through structured strategies. Key takeaway? Mental health care is essential – neglecting it risks worsening both. Even between attacks, 20% struggle with cognitive fog affecting work and relationships.
Ready to break this cycle? Managing your daily life with migraine means understanding these hidden connections. Good news? Recognizing these patterns reveals holistic treatment strategies that address physical and mental health – from workplace flexibility to therapies targeting brain chemistry directly.
Taking Control: Management Strategies And Finding Hope
Building Your Management Toolkit
Effective migraine management combines acute treatments (to stop attacks) and preventive treatments (to reduce frequency). Lifestyle adjustments like consistent sleep, stress management, and hydration form the foundation of care. Working closely with healthcare providers ensures personalized solutions work best for your unique needs. Identifying triggers through a migraine journal can significantly reduce attacks.
Acute treatments include over-the-counter pain relievers for mild episodes and triptans (almotriptan, zolmitriptan) for severe attacks. Newer options like CGRP inhibitors (ubrogepant) offer alternatives, especially for cardiovascular patients. Tracking attacks helps identify patterns and medication effectiveness—70% of patients improve after optimizing hydration and stress-reduction techniques.
Empowerment Through Knowledge And Advocacy
Becoming an expert in your condition transforms your relationship with migraines. Open communication with doctors optimizes treatment plans, while sharing experiences with loved ones builds support networks. Research advances mean new therapies emerge regularly, offering hope for better management. Anti-CGRP treatments now provide monthly injections reducing attack days by 50% in clinical trials.
Non-drug approaches like biofeedback and cognitive behavioral therapy complement medication. Staying informed about clinical trials and advocating for accommodations strengthens control. Remember: 60% of patients achieve major improvement through tailored approaches. Tools to track symptoms empower data-driven decisions with your doctor.
Migraine is a neurological condition shaped by genetics, brain chemistry, and triggers. Understanding phases and patterns enables effective management. Tailored treatments, lifestyle changes, and medical care offer relief. Track symptoms, use research advances—hope exists. Proactive steps and support help reclaim control, showing migraine doesn’t define your life.
FAQ
What causes migraines?
Migraines arise from a complex interplay of genetic, neurological, and environmental factors. Research shows they’re strongly linked to genetics—about 70% of migraineurs have a close relative with the condition. Brain chemicals like serotonin and CGRP (Calcitonin Gene-Related Peptide) also play a role. For example, serotonin levels drop during an attack, potentially contributing to pain, while CGRP causes inflammation and intense pain when released around brain nerves. The trigeminal nerve, a major pain pathway, is activated during attacks, reinforcing that migraines are a neurological disease, not just a vascular issue. Triggers like stress, hormonal shifts, or sensory stimuli act as “spark plugs” for those with this underlying sensitivity. Harvard Health highlights this genetic connection.
Is migraine dangerous?
While migraines themselves aren’t typically life-threatening, they can increase stroke risk slightly—especially for people with aura. However, this risk remains low overall. The bigger danger lies in their impact on daily life: chronic pain, missed work, or mental health challenges like anxiety and depression are common. Migraines aren’t “just a headache”; they’re a disabling neurological disease recognized by the WHO as a primary headache disorder. If you experience sudden, severe headaches or new neurological symptoms (e.g., weakness, speech issues), seek immediate medical help to rule out other causes. WHO emphasizes their global health impact.
How is a migraine different from a regular headache?
Migraines and tension headaches differ in severity, symptoms, and impact. Migraines cause moderate-to-severe, throbbing pain usually on one side of the head, worsened by activity. They’re paired with nausea, vomiting, and extreme sensitivity to light/sound. Tension headaches, however, feel like a dull, bilateral pressure with mild-to-moderate pain that doesn’t disrupt daily life. Migraines are also more likely to include aura (visual disturbances) and can last 4–72 hours untreated, while tension headaches rarely exceed 72 hours. Think of migraines as a full-body neurological event versus a localized muscle-tension issue.
Can migraines be cured?
There’s no cure yet, but treatments can significantly reduce frequency and severity. Acute medications like triptans stop attacks in progress, while preventives (beta-blockers, CGRP inhibitors) cut long-term risk. Lifestyle adjustments—regular sleep, hydration, stress management—are equally vital. For chronic migraines (15+ headache days/month), combining medication and behavioral changes often helps. Though migraines are lifelong, many find their symptoms improve over time with proper care. The key is working with a doctor to build a personalized “toolkit” for managing triggers and attacks exploring the different types of migraines.
How can I stop a migraine quickly?
Act fast when symptoms start. Over-the-counter NSAIDs (ibuprofen, aspirin) work well for mild cases. For stronger attacks, triptans (sumatriptan) or gepants (ubrogepant) target CGRP to halt pain. Rest in a dark, quiet room—sensory overload worsens symptoms. Cold compresses, hydration, or caffeine (in moderation) may help. If attacks recur, talk to your doctor about preventive options. Newer therapies like neuromodulation devices (e.g., Cefaly) offer non-drug relief by stimulating nerves to disrupt pain signals.
How do I know if I have a migraine?
Look for these red flags: throbbing, one-sided pain worsened by movement, plus nausea or sensory sensitivity. The “rule of five” applies—diagnosis requires at least five attacks matching these criteria. Keeping a migraine diary helps track patterns (frequency, duration, triggers) for your doctor. Imaging tests like MRIs rule out other causes but don’t diagnose migraines directly. If you experience aura (flashing lights, blind spots) or postdrome fatigue afterward, that’s another clue. For personalized guidance, consult a neurologist or use a the full sequence of migraine symptoms to decode your experiences.
Can migraines cause a stroke?
Migraines, especially with aura, slightly raise stroke risk. Studies show people with aura have a 2–3x higher chance of ischemic stroke compared to those without. However, the absolute risk remains very low—about 1 in 100,000 migraineurs under 45 will have a stroke. Risk factors like smoking, estrogen use, or high blood pressure compound this risk. To stay safe, avoid smoking, manage cardiovascular health, and discuss preventive strategies with your doctor if you have aura. Remember, migraines are more likely to affect quality of life than cause stroke.
How long does a migraine attack last?
Untreated attacks typically last 4–72 hours, but duration varies. With treatment, they often resolve faster. Chronic migraineurs (15+ headache days/month) may experience near-constant pain. The four phases—prodrome, aura, attack, postdrome—each contribute to the timeline. For example, prodrome symptoms (mood changes, neck stiffness) may start 24–48 hours before pain, while postdrome fatigue lingers 24–48 hours after. Keeping a diary helps predict patterns and tailor treatment managing your daily life with migraine.
What are the four stages of a migraine?
1. Prodrome: One to two days before pain, you might feel irritable, crave foods, or notice neck stiffness. 2. Aura (not everyone): Visual disturbances (flashing lights, blind spots) or sensory issues (tingling, speech trouble) develop over 5–60 minutes. 3. Attack: The headache phase brings throbbing pain, nausea, and sensitivity to light/sound, lasting 4–72 hours. 4. Postdrome: Post-attack “hangover” leaves you drained, with possible brief pain relapses from sudden movement. Each phase varies—some skip aura, others experience all. Understanding these stages helps you anticipate and manage symptoms understanding your specific migraine causes and triggers.