Exploring the different types of migraines
The key takeaway: Migraine is a complex neurological disease, not just a headache, with over 300 headache types but distinct phases (prodrome, aura, attack, postdrome) and subtypes like migraine with/without aura. Recognizing these helps tailor treatment. According to WHO, headaches affect ~40% of people globally, but migraine alone impacts 1 in 7, emphasizing its widespread yet misunderstood burden.
Are migraines leaving you confused and frustrated, unsure why your symptoms don’t fit the “classic” picture? This article breaks down the diverse types of migraines, from the common migraine without aura to rare forms like hemiplegic migraine (mimicking stroke-like symptoms) or retinal migraine (causing temporary vision loss in one eye). You’ll uncover how these neurological conditions uniquely impact your body by exploring phases like the prodrome (early warnings) and postdrome (“migraine hangover”), revealing hidden triggers, silent symptoms, and why some migraines strike without head pain (silent migraines). By understanding nuances—from chronic migraines affecting 15+ days/month to dizziness-linked vestibular migraines—you’ll gain clarity to better communicate with doctors and take back control.
- Understanding migraine: more than just a headache
- The Four Phases Of A Migraine Attack
- The Two Primary Types: Migraine With Aura vs. Without Aura
- Exploring Other Specific Types of Migraine
- Chronic migraine: when attacks become frequent
- The migraine pain spectrum: how severe can it get?
- A Special Focus on Migraines in Children
- Navigating the diverse world of migraines
Understanding migraine: more than just a headache
Migraine isn’t just a headache – it’s a complex neurological disease affecting over 1 billion people worldwide. Recognized by the World Health Organization as the second leading cause of disability globally, this condition causes more than temporary discomfort. Unlike common headaches, migraines involve neurological processes that can dramatically impact daily life.
What is a migraine?
Defined by Inserm as a chronic neurological disease, migraines manifest through recurring attacks rather than occasional discomfort. These episodes stem from complex brain activity involving nerve pathways and chemicals like CGRP (calcitonin gene-related peptide). During an attack, brain cells communicate abnormally, triggering the characteristic pain and associated symptoms.
Key facts to understand this condition:
- Second leading cause of disability worldwide
- Typical duration: 4-72 hours per episode
- Affects 18% of women vs. 6% of men annually
- More prevalent among socioeconomically disadvantaged groups
Migraines vs. other headaches
While over 300 headache types exist, migraines stand apart from common tension-type headaches described by Harvard Health. The latter feel like a “tight band” around the head, lasting 30 minutes to 7 days without pulsing pain or activity aggravation. Crucially, migraines involve neurological symptoms beyond pain.
Headache disorders affect 40% of the global population – that’s 3.1 billion people. While tension headaches dominate prevalence (78% of adults), migraines cause disproportionate disability. Unlike sinus headaches or medication-overuse headaches, migraines involve specific neurological phases: prodrome, aura, attack, and postdrome.
Understanding these distinctions matters because types of migraines vary significantly in symptoms and management needs. The following sections will explore these differences to help identify when head pain might indicate a more complex neurological event rather than a simple headache.
The Four Phases Of A Migraine Attack
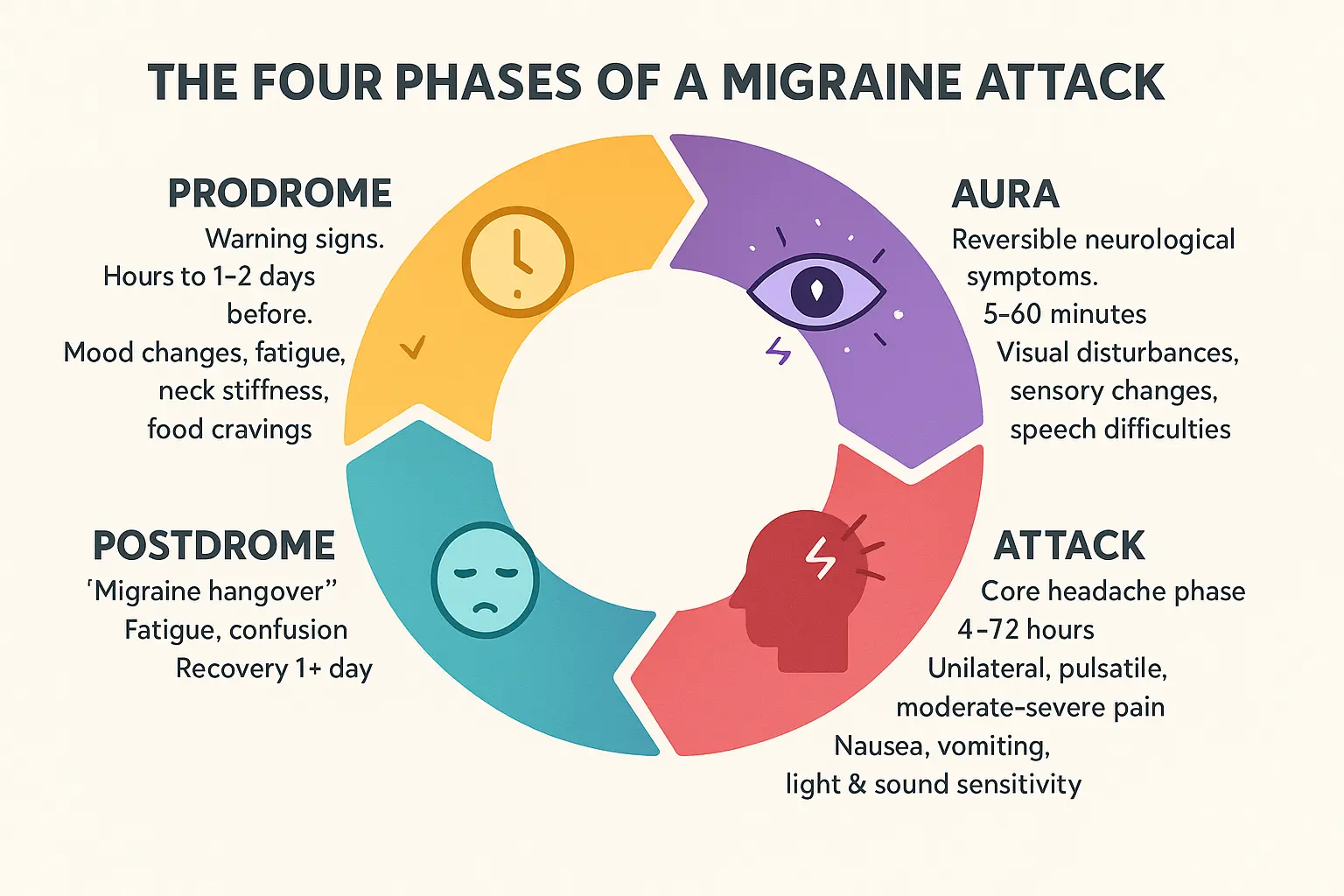
The Prodrome: The Warning Signs
Up to 60% of migraine sufferers experience prodrome, an early warning phase occurring hours or even days before a headache. This phase acts like a “canary in the coal mine” with subtle clues like:
- Mood shifts (irritability or euphoria)
- Neck stiffness and muscle tension
- Altered food cravings
- Sleep disturbances
- Increased urination
Recognizing these signs creates a critical window for intervention. We recommends tracking symptoms through apps to identify personal patterns. Simple measures like hydration and avoiding known triggers during this phase can sometimes prevent full-blown attacks. For instance, magnesium-rich foods like almonds or a warm compress on the neck might ease early symptoms. Prodromal symptoms often resemble pre-menstrual tension in women, which explains why hormonal changes frequently trigger migraines.
The Aura: Temporary Neurological Symptoms
About 25% of migraineurs experience aura, a neurological storm lasting 5-60 minutes. Visual disturbances dominate:
- Seeing shimmering lights or zigzag patterns
- Temporary vision loss (scotoma)
- Pulsing or flickering lights
Additional symptoms include:
- One-sided numbness or tingling
- Speech difficulties (dysarthria)
- Less commonly: Hearing changes or vertigo
These symptoms stem from cortical spreading depression, a wave of electrical activity across the brain. Pain pathways are activated while causing temporary sensory disruptions. Aura can occur without headache (acephalgic migraine) or during the headache phase. Visual auras often start as small blind spots that expand slowly – imagine looking through a cracked windshield. This phase feels like a “brain short-circuit” where sensory overload makes even quiet environments unbearable.
The Attack: The Headache Phase
This defining phase brings:
- Throbbing, one-sided pain
- Aggravation through physical activity
- Photophobia (light sensitivity) and phonophobia (sound sensitivity)
- Nausea or vomiting
Attacks typically last 4-72 hours. The International Headache Society emphasizes this phase requires at least two of these characteristics for diagnosis. Routine tasks become challenging – 90% report reduced productivity. The pain often starts behind one eye (retro-orbital) and spreads, with 60% experiencing one-sided symptoms throughout. Sensory overload explains why migraineurs retreat to dark, quiet rooms – even a gentle breeze on the face can trigger pain. During this phase, 40% experience allodynia where a simple hair brushing becomes agonizing.
The Postdrome: The “Migraine Hangover”
Over 80% endure this recovery phase lasting hours to days. Symptoms mirror a physical hangover:
- Exhaustion or paradoxical energy surges
- Brain fog and concentration issues
- Body aches and neck stiffness
- Continued light/sound sensitivity
Postdromal symptoms often mimic pre-attack signs. Management focuses on recovery – stretching, hydration, and avoiding bright screens. If symptoms persist beyond 48 hours, medical consultation becomes crucial. Many patients report appetite swings during this phase – going from zero hunger to extreme cravings. This phase often brings emotional volatility too, with 30% experiencing postdromal depression despite physical pain relief. The “migraine hangover” creates a catch-22: needing rest but struggling to sleep due to lingering sensory sensitivity.
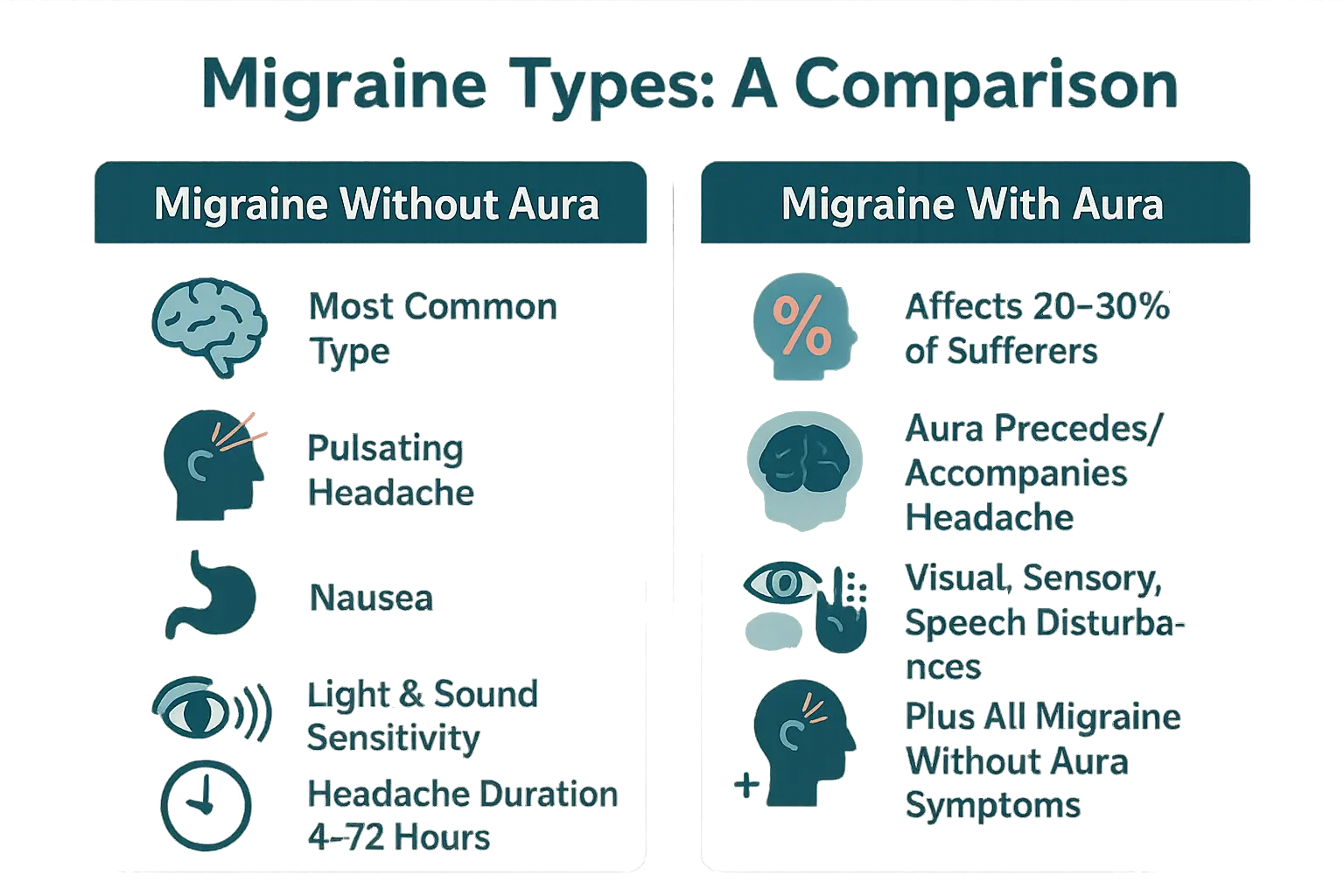
The Two Primary Types: Migraine With Aura vs. Without Aura
Migraine Without Aura: The Most Common Form
Migraine without aura affects approximately 80% of people with migraines. It causes moderate to severe headaches lasting 4 to 72 hours. Symptoms include pulsating pain, typically on one side of the head, worsened by physical activity. Nausea, vomiting, and sensitivity to light (photophobia) or sound (phonophobia) often accompany the pain. Despite lacking neurological disturbances like aura, this type includes prodrome and postdrome phases with mood changes, fatigue, or light sensitivity before or after the headache.
Triggers like stress, hormonal changes, or dietary factors are common. Common dietary triggers include chocolate, aged cheeses, or monosodium glutamate. Diagnosis uses clinical criteria, focusing on duration, location, and symptoms. Management combines acute treatments like NSAIDs or triptans with preventive strategies such as lifestyle adjustments. Tracking triggers and maintaining regular sleep and hydration can reduce frequency.
Migraine With Aura: When the Headache Is Announced
About 20-30% of migraine sufferers experience aura, a temporary neurological disturbance before or during the headache. Visual symptoms are most common, such as flashing lights, zigzag lines, or blind spots. Other auras may involve sensory issues (numbness), speech difficulties, or motor weakness. These symptoms develop gradually over 5-60 minutes and resolve before or during the headache.
This type is linked to cortical spreading depression, a wave of brain activity altering nerve cells. It carries a slightly increased stroke risk, especially for younger women using hormonal contraceptives. The risk arises because estrogen in contraceptives can exacerbate clotting tendencies, which combine with aura-related vascular changes. Though sometimes called “ophthalmic migraine,” “migraine with aura” is the medical standard. Some individuals alternate between aura and non-aura migraines.
For more details on other migraine forms, many forms exist beyond these two primary types.
At a Glance: Comparing the Two Main Types
| Feature | Migraine Without Aura | Migraine With Aura |
|---|---|---|
| Presence of Aura | No | Yes (precedes or accompanies the headache) |
| Frequency | 80% of migraine cases | 20-30% of migraine cases |
| Key Symptoms | Pulsating headache, nausea, photophobia, phonophobia | All symptoms of migraine without aura, plus temporary visual, sensory, or speech disturbances |
| Typical Duration of Headache Phase | 4 to 72 hours | 4 to 72 hours |
Understanding these distinctions helps patients and healthcare providers tailor treatment. For example, migraine with aura may require additional stroke risk assessments. Both types benefit from trigger avoidance and acute medications like NSAIDs, though triptans are generally avoided during aura symptoms. Shared risk factors like stress or sleep disturbances allow holistic strategies such as stress-reduction techniques, hydration, and consistent sleep routines. Always consult a specialist for personalized care.
According to Inserm, migraine with aura affects 20-30% of sufferers. This distinction underscores the importance of accurate diagnosis for effective management, as shared risk factors like stress or sleep disturbances allow holistic strategies applicable to both types.
Exploring Other Specific Types of Migraine
Migraine Aura Without Headache (Silent Migraine)
Silent migraines involve aura symptoms—like flashing lights, tingling, or speech difficulties—without a headache. These episodes, lasting 5–60 minutes, disrupt daily life despite lacking pain. They’re often overlooked but recognized as valid neurological events. Symptoms may also include fatigue, nausea, or light sensitivity without visual changes. Research confirms these disruptions are real, like impaired concentration or phantom limb sensations. For example, temporary numbness in one hand during a work meeting could hinder productivity. Diagnosis requires understanding this subtype’s legitimacy and ruling out stroke or transient ischemic attacks (TIAs).
Hemiplegic Migraine: A Rare and Alarming Form
Hemiplegic migraine causes temporary one-sided body weakness, mimicking stroke. It has two forms: familial (FHM), linked to CACNA1A, ATP1A2, or SCN1A gene mutations, and sporadic (SHM), without family history. These genetic disruptions cause abnormal ion transport, leading to brain hyperexcitability. Weakness follows visual or sensory auras and can last hours to days—far longer than typical aura. For instance, a person might lose the ability to use their right arm for a day. Diagnosis involves genetic testing (for FHM) or ruling out other causes (for SHM). Given the stroke-like symptoms, immediate medical evaluation is critical to avoid misdiagnosis.
Retinal Migraine: When Vision Is Affected in One Eye
Retinal migraines cause temporary vision loss in one eye—scintillations, blind spots, or blindness—lasting 5–60 minutes. Unlike typical visual auras (which affect both eyes), these disturbances are monocular. For example, someone might report, “My left eye went completely black while reading.” Urgent evaluation is key to exclude retinal artery occlusion or embolism. Diagnosis requires strict criteria: unilateral visual disturbances followed by headache within 60 minutes, with other causes ruled out. Though rare, untreated cases pose risks like permanent vision loss, highlighting the need for urgent action.
Migraine With Brainstem Aura
Formerly called basilar-type migraine, this subtype causes brainstem-origin symptoms like:
- Slurred speech (dysarthria)
- Vertigo or tinnitus (ringing in ears)
- Hearing loss (hypoacusis)
- Double vision (diplopia)
- Balance loss (ataxia)
- Reduced consciousness
These occur with or without headache but no motor or retinal symptoms. Diagnosis requires excluding strokes or mitochondrial disorders, especially in children who may be misdiagnosed with a seizure due to confusion and dizziness without pain. Unlike hemiplegic migraine, no muscle weakness occurs. Accurate diagnosis hinges on neurological exams and imaging to rule out structural causes.
Vestibular Migraine: When Dizziness Takes Center Stage
Vestibular migraines feature dizziness or vertigo lasting 5 minutes to 72 hours, with or without headache. Diagnosis relies on migraine history and vestibular symptoms (e.g., motion-induced vertigo) plus photophobia or phonophobia. For example, a patient might experience spinning sensations when turning their head. No specific biomarkers exist, so inner-ear disorders like Meniere’s disease are ruled out first. Triggers include stress, hormonal shifts, or visual stimuli like flickering lights. Treatment combines migraine medications (e.g., beta-blockers) and vestibular rehab, including balance exercises. Unlike other subtypes, symptoms can strike unpredictably, affecting driving or work performance.
Recognizing these subtypes enables targeted care. Hemiplegic migraine’s genetic link highlights family screening, while retinal migraine’s vascular risks demand urgent evaluation. If unusual neurological symptoms occur without pain, consult a specialist—these conditions are treatable and distinct from transient ischemic attacks or anxiety. For rare subtypes like hemiplegic migraine, genetic testing at Inserm may reveal actionable insights. Accurate diagnosis helps manage life with fewer disruptions.
Chronic migraine: when attacks become frequent
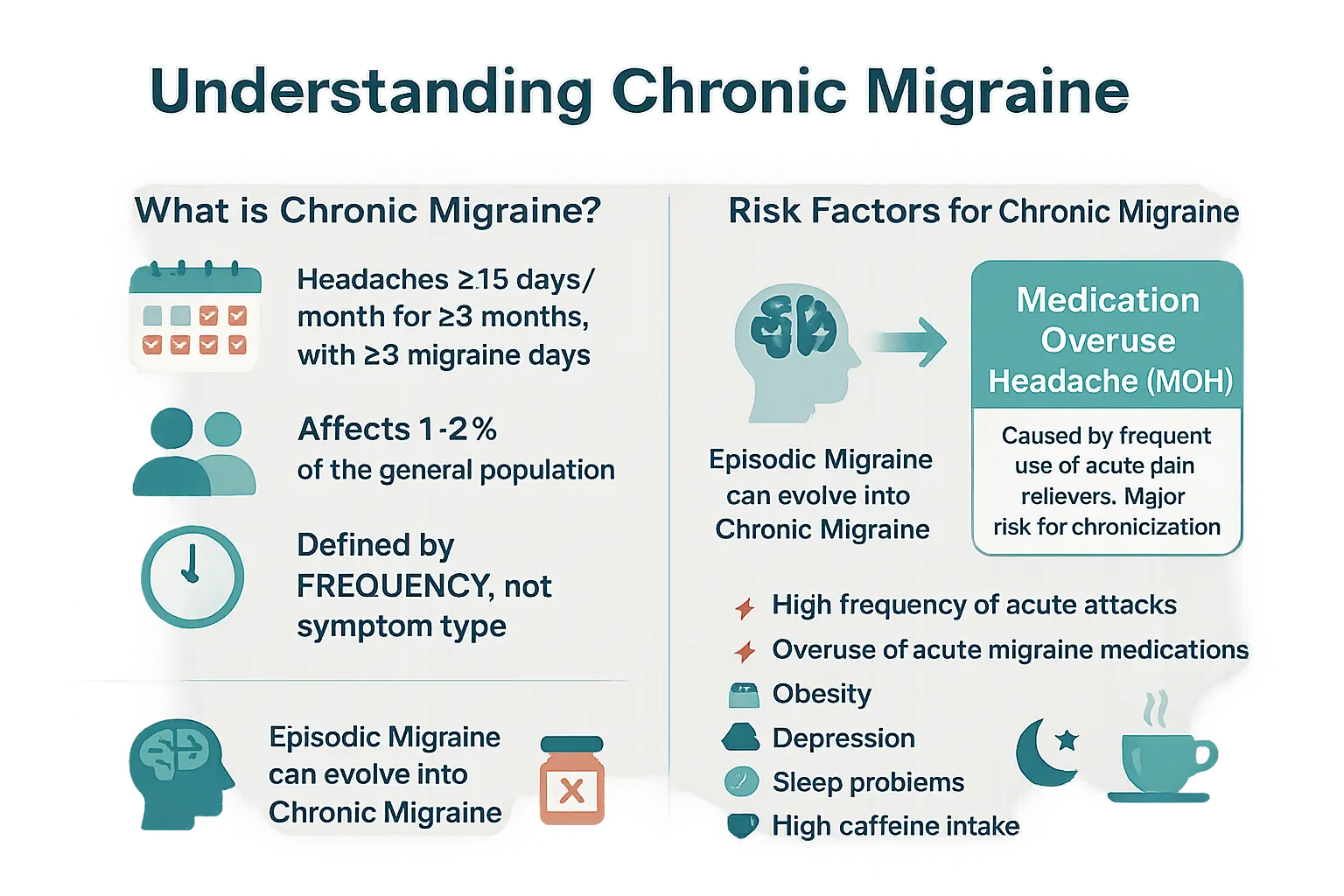
Defining chronic migraine
Chronic migraine affects 1-2% of the global population, according to Inserm. It’s diagnosed when headaches occur 15+ days/month for 3+ months, with at least 8 migraine days/month. Unlike other types, frequency—not symptom severity—defines it. Pain may mimic migraines or tension headaches. About 5% of episodic migraine sufferers transition to chronic annually, underscoring the need for early intervention. This condition profoundly impacts daily life, affecting work, relationships, and overall quality of life. Per the Global Burden of Disease Study (GBD2015), it ranks as the third most disabling disease for under-50s worldwide.
Risk factors and the link to medication overuse
Chronic migraine often evolves from episodic migraine. Key risks include:
- High attack frequency
- Medication overuse
- Obesity
- Depression
- Sleep disorders
- Excess caffeine
For instance, obesity increases inflammation and hormonal imbalances, which may overactivate migraine pathways. Depression and sleep disorders like insomnia disrupt neurotransmitter balance, lowering pain thresholds. Women face higher risks due to hormonal shifts like menstrual cycles or menopause.
Medication overuse headache—a WHO-cited factor—worsens symptoms. Using triptans/NSAIDs >8 days/month raises chronic risk by 5% yearly. Common culprits include ergotamines, codeine, and combination analgesics. Stopping overused meds can halve headache frequency for some patients, per studies.
Management prioritizes prevention. Doctors often recommend headache diaries to track triggers and medication use. Preventive therapies include CGRP inhibitors, beta-blockers, anticonvulsants like topiramate, or antidepressants like amitriptyline. Lifestyle changes—regular sleep, hydration, caffeine reduction—are critical. For severe cases, supervised detox under medical guidance helps reset pain pathways. Addressing comorbidities like sleep apnea or depression improves outcomes. Early diagnosis and multidisciplinary care—neurology, psychology, lifestyle adjustments—offer the best hope for reducing disability.
The migraine pain spectrum: how severe can it get?
Is there a “most painful” type of migraine?
Migraine pain perception varies dramatically between individuals. No single type qualifies as “most painful,” though all forms cause debilitating suffering. Scientific studies show pain thresholds and intensity ratings depend on brain sensitivity, stress levels, and sleep patterns.
Subtypes like hemiplegic migraine cause alarming neurological symptoms (temporary weakness) while ocular migraine creates vision disturbances. However, these manifestations don’t necessarily correlate with increased pain intensity. Vestibular migraines add vertigo to typical symptoms, creating disorienting episodes that challenge daily functioning despite similar pain levels to other subtypes.
Distinguishing migraine from cluster headaches
Cluster headaches, classified as trigeminal autonomic cephalalgias by the WHO, feature excruciating eye-orbital pain lasting 15-180 minutes. Unlike migraines, they occur in cyclical clusters (multiple daily episodes for weeks) followed by remission periods. These attacks affect 0.1% of people globally – six times more men than women – and often begin before age 30.
Differentiators include:
- Unilateral orbital pain vs migraines’ variable location
- Autonomic symptoms: eye redness, nasal congestion, eyelid swelling
- Agitation during attacks (migraineurs prefer stillness)
- Circadian pattern – attacks often wake sufferers at consistent times
Though migraines affect 1 in 7 people globally, cluster headaches strike 0.1% – yet sufferers rate their pain as “suicide headaches.” Alcohol triggers cluster attacks, unlike migraines with individualized dietary factors. The WHO emphasizes these headaches represent a major public health burden, often misdiagnosed as dental/sinus issues.
Explore other intense headaches for comparable pain profiles requiring distinct treatments.
A Special Focus on Migraines in Children
Recognizing Childhood Migraines
Migraines in children often differ from adult cases, complicating diagnosis. Unlike adults’ one-sided pain, kids frequently report bilateral headaches with a compressive sensation. Symptoms like pale skin, dark under-eye circles, and abdominal pain may replace head pain entirely. Young children often struggle to articulate visual or sensory changes linked to migraines with aura, risking misdiagnosis as stomach issues.
Episodes typically last 2-4 hours—shorter than in adults—with sleep often providing relief. Up to 10% of children experience migraines, yet many cases go unnoticed due to atypical symptoms. Disrupted playtime affects 84% of these children, while 40% endure vomiting.
Abdominal Migraine and Cyclic Vomiting Syndrome
Abdominal migraines affect 4% of children, causing midline stomach pain (2-72 hours) and nausea/vomiting without headaches. This “migraine equivalent” evolves into classic migraines for 50% of cases by adulthood. Diagnosis involves excluding digestive disorders via Dignan’s criteria, focusing on functional impairment and symptom-free intervals.
Cyclic vomiting syndrome shares migraine links, featuring predictable vomiting episodes (8-24 hours) with full recovery between crises. Stress or dietary triggers overlap with migraines, and treatments like propranolol address both. Early intervention is key to prevent progression.
Persistent symptoms require pediatric neurology evaluation to avoid academic disruption.
Navigating the diverse world of migraines
Understanding migraines requires recognizing they are not a single condition but a spectrum of neurological disorders, each with unique traits. From common types like migraine without aura to rarer forms like hemiplegic migraine, symptoms vary widely.
Accurate diagnosis is critical. Only a healthcare professional can distinguish between migraine types and rule out secondary causes—like infections, tumors, or vascular issues—that demand urgent care. Ignoring severe symptoms (e.g., sudden “thunderclap” headaches, vision loss, or neurological deficits) could delay life-saving treatment.
Self-diagnosis risks mismanagement. For instance, retinal migraines (affecting one eye) might mimic stroke, while chronic migraines (15+ headache days/month) require tailored strategies to prevent progression. Early consultation ensures personalized care, reducing disability and improving quality of life.
If migraines disrupt your daily routine or present unusual symptoms, seek medical advice. A neurologist or headache specialist can decode your specific pattern, recommend evidence-based therapies, and guide preventive measures. Your health—and clarity—is worth it.
Migraine isn’t a single condition but a neurological disorder spectrum with varied types and symptoms. Common types include migraine with/without aura; rare ones like hemiplegic or vestibular migraine require specific approaches. Recognizing symptoms, tracking patterns, and consulting a doctor are key steps for effective care and better quality of life.
FAQ
What are the main types of migraines?
Migraines come in various forms, but the two primary categories are migraines with aura and migraines without aura. About 80-85% of migraine sufferers experience attacks without aura, characterized by pulsing, one-sided headaches lasting 4-72 hours, often accompanied by nausea, light sensitivity (photophobia), or sound sensitivity (phonophobia). Migraines with aura affect 20-30% of patients and include temporary neurological symptoms like visual disturbances (e.g., flashing lights), tingling sensations, or speech difficulties before or during the headache phase. Other subtypes, like hemiplegic migraine (with temporary weakness) or retinal migraine (affecting one eye), are rarer. Always consult a healthcare provider for proper diagnosis.
Which migraine type causes the most intense pain?
Pain perception varies greatly between individuals, but hemiplegic migraine is often described as particularly debilitating due to its alarming symptoms like temporary paralysis on one side of the body. However, the most severe pain is commonly associated with cluster headaches, though these aren’t technically migraines. Cluster headaches cause excruciating, one-sided pain around the eye, lasting 15 minutes to 3 hours, and occur in clusters over weeks or months. While migraines can be intensely painful, cluster headaches are often cited as among the worst human pain experiences. The International Headache Society classifies cluster headaches separately, emphasizing their unique treatment needs.
What are the 4 C’s for managing migraines?
The “4 C’s” aren’t a medically standardized acronym, but they might refer to key aspects of migraine care: Coping strategies (like stress reduction), Consistency in sleep and meal patterns to avoid triggers, Communication with healthcare providers about symptoms, and Careful medication use to prevent overuse headaches. For example, maintaining regular sleep patterns (consistency) reduces risk by 20-30%, while medication overuse contributes to chronic migraines in 5-10% of cases. Always consult a neurologist for personalized management plans.
Can migraines cause ear pain?
While migraines don’t directly cause ear pain, some subtypes can create related sensations. Vestibular migraines may include ear-related symptoms like tinnitus (ringing), hearing changes, or a feeling of fullness in the ear. Migraine with brainstem aura (formerly basilar-type) can cause temporary hearing loss or vertigo. However, persistent ear pain should be evaluated separately, as it might indicate conditions like temporomandibular joint (TMJ) issues or ear infections. A 2021 study found 12% of vestibular migraine patients reported ear pressure during attacks, highlighting the importance of differential diagnosis.
What happens during the fourth phase of a migraine attack?
The fourth and final stage, called the postdrome, occurs after the headache subsides. About 80% of migraineurs experience this “migraine hangover,” which can last hours to two days. Common symptoms include fatigue, brain fog, body aches (especially in the neck/shoulders), and sensitivity to light/sound. Some people feel euphoric, while others experience mood swings. Recovery requires rest, hydration, and avoiding triggers. Keeping a migraine journal helps identify patterns—60% of patients report better management after tracking postdrome symptoms.
What are the seven most common headache categories?
While there are over 300 headache types, the seven most prevalent include: 1. Tension-type headaches (78% of cases) 2. Migraines (15% prevalence) 3. Cluster headaches (0.1% incidence) 4. Sinus headaches (3% association with infections) 5. Medication-overuse headaches (1-2% of chronic cases) 6. Trigeminal neuralgia (0.01% prevalence) 7. Exertional headaches (1% during physical activity) Migraines stand out for their neurological symptoms and disability—accounting for 50% of days lost to headache disorders globally, per WHO data.
Which migraine type is the rarest?
Hemiplegic migraine affects fewer than 1 in 1,000 migraineurs, making it one of the rarest. This subtype causes temporary motor weakness on one side of the body during aura, often mistaken for stroke. Familial hemiplegic migraine (FHM), linked to genetic mutations like CACNA1A, accounts for 30% of cases. Symptoms typically begin before age 20. Though less common than typical migraines, hemiplegic attacks require specialized care due to their stroke-like presentation and potential complications like status migrainosus (attacks lasting >72 hours).
What’s the most severe pain humans experience?
While migraines can be extremely painful, cluster headaches are often described as the most severe. Classified by the ICD-11 as “suicide headaches,” these attacks cause orbital pain scoring 8-10 on the 10-point scale, lasting 15 minutes to 3 hours. They occur in cycles, sometimes multiple daily, and affect 0.1% of the population. Other contenders include trigeminal neuralgia (nerve pain) and childbirth. Importantly, chronic migraine (≥15 headache days/month) affects 1-2% of people globally and can be equally disabling long-term, even if individual attacks feel less intense.
Is there a permanent cure for migraines?
Currently, there’s no permanent cure for migraines, but effective management options exist. Preventive medications like erenumab reduce attack frequency by 50% in 40% of patients. Acute treatments (triptans, gepants) stop attacks early. Lifestyle modifications—such as maintaining regular sleep (reduces frequency by 30%), hydration, and trigger avoidance—also help. For chronic cases, neuromodulation devices or Botox injections provide relief. The WHO emphasizes multidisciplinary approaches, combining pharmacological and non-pharmacological methods. While not curable, 50% of patients achieve significant improvement through personalized treatment plans developed with headache specialists.