Essential takeaways: Beyond migraines, 300+ headache types affect 40% globally (WHO), mostly primary. Cluster headaches cause intense eye pain in cycles; cervicogenic ones link to neck issues. Accurate diagnosis ensures targeted care—from emergency treatment for thunderclap headaches to physiotherapy. Recognizing these variations improves pain management and quality of life.
Ever experienced a headache that didn’t fit the usual migraine or tension type? You’re not alone—other headaches include over 300 types, often overlooked yet impactful. From cluster headaches (“suicide headaches” with searing, one-sided eye pain) to thunderclap headaches requiring urgent care, these affect 40% of people globally, per the WHO, yet remain underestimated and undertreated. This article demystifies lesser-known other headaches—like cervicogenic headaches (neck-related pain) or exertion-triggered types—and explains primary (standalone) vs. secondary (symptom of another condition) causes. Get clear insights to decode your pain and find targeted relief, no medical jargon, just practical guidance.
- Beyond migraine: exploring the world of other headaches
- A closer look at other primary headaches
- When headaches are a symptom: understanding secondary headaches
- Headaches In Specific Populations: Children And Pregnancy
- Red flags: when to see a doctor immediately
- How are other headaches diagnosed?
- Navigating treatment and prevention for other headaches

Beyond migraine: exploring the world of other headaches
Most people associate headaches with migraines and tension headaches. Yet over 300 types exist, affecting 40% of the global population. These often go untreated despite causing disability and economic costs. Understanding primary vs secondary headaches is key: primary headaches aren’t symptoms of other conditions – they’re the condition itself. Secondary headaches indicate underlying issues like infections or brain hemorrhages. Primary types account for 90% of cases, but secondary ones require urgent care.
What are primary headaches?
These headaches originate independently. Common types include:
- Cluster headaches – Severe, one-sided pain with tearing, affecting men six times more than women.
- Medication overuse headaches – Caused by excessive painkiller use, impacting up to 5% of some populations.
- Trigeminal autonomic cephalalgias – Rare, intense headaches like paroxysmal hemicrania requiring specific treatments.
Though non-life-threatening, they disrupt daily life. Treatments range from OTC painkillers to targeted medications.
What are secondary headaches?
These headaches signal underlying health problems. Red flags include sudden severe pain, changes after age 50, or neurological symptoms. Causes span:
- Structural issues – Brain hemorrhages, tumors, or sinus infections.
- Systemic conditions – Hypertension or chronic diseases.
- Medication effects – Including post-lumbar puncture headaches.
Seek immediate care for “thunderclap” headaches or vision changes. Treating the root cause – whether infection or structural abnormality – typically resolves the pain. Early detection remains critical for these potentially serious conditions.
A closer look at other primary headaches
While migraine and tension headaches dominate public awareness, understanding rare primary headache types improves diagnostic accuracy. These aren’t linked to underlying diseases but significantly impact quality of life. Let’s examine key variations and why recognition matters – particularly when differentiating primary from secondary headaches that signal serious conditions.
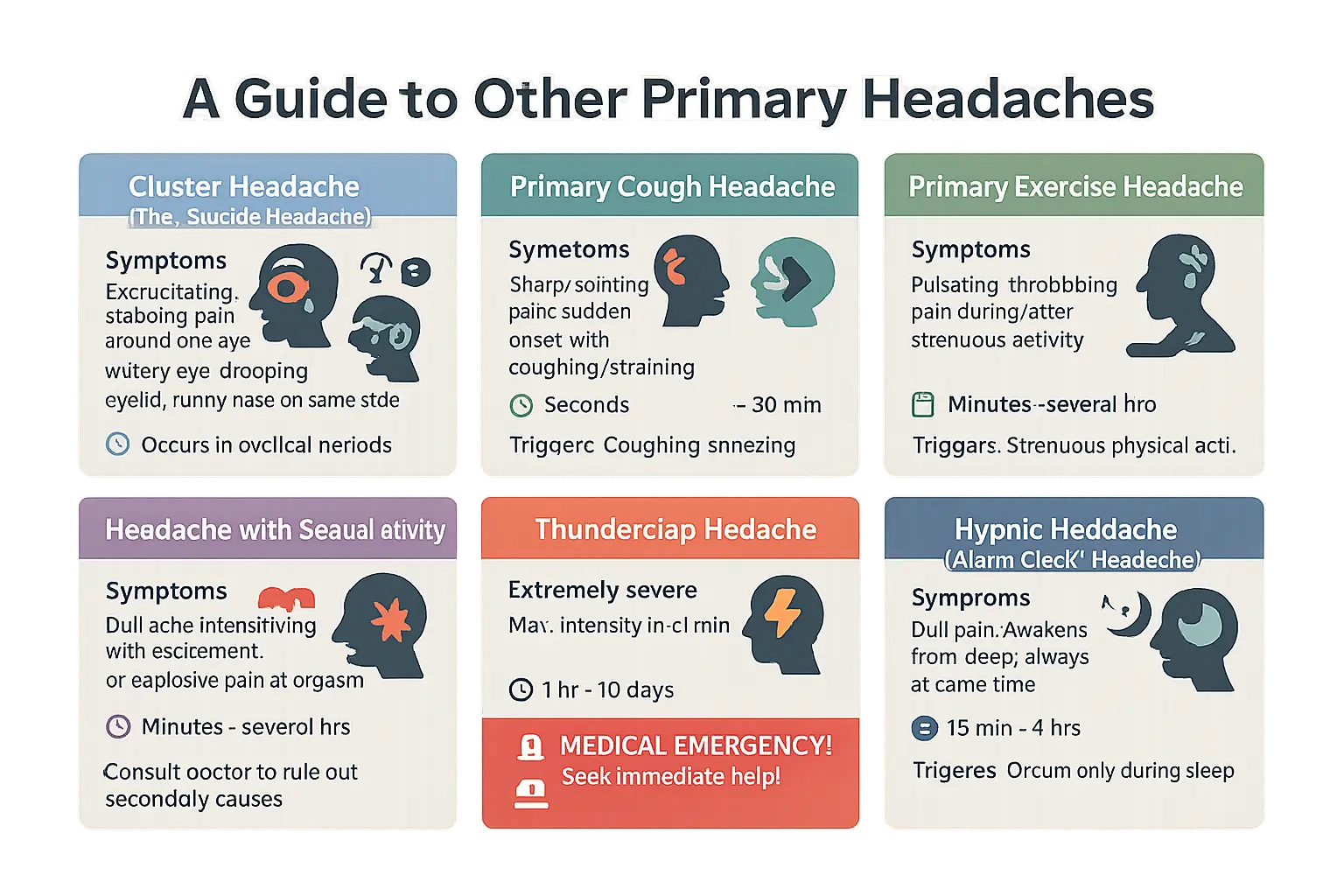
| Headache Type | Key Symptoms | Duration | Common Triggers |
|---|---|---|---|
| Cluster Headache | Excruciating one-sided eye pain with tearing, runny nose, or drooping eyelid (Horner syndrome in some cases) | 15 mins to 3 hours during cyclical episodes | Alcohol, smoking, sleep pattern changes |
| Primary Cough Headache | Sharp pain during coughing, sneezing, or straining | Seconds to 30 minutes | Respiratory strain, bowel movements |
| Primary Exercise Headache | Pulsing head pain during intense activity | Minutes to 48 hours | Strenuous exercise |
| Sexual Activity Headache | Dull ache worsening with arousal or explosive pain at orgasm | Minutes to hours | Orgasm |
| Thunderclap Headache | Worst pain instantly, peaks in <1 minute | 1 hour to 10 days | Medical emergency |
| Hypnic Headache | Dull nighttime pain waking at same time | 15 mins to 4 hours | Occurs during sleep |
Cluster headache: the “suicide headache”
Named for their cyclical nature, cluster headaches cause severe one-sided eye pain with tearing, nasal congestion, and restlessness. Attacks occur in clusters lasting weeks or months, followed by remission periods. Risk factors include alcohol, smoking, and irregular sleep. Affecting 1 in 1,000 people (Migraine Quebec), this condition typically strikes adults 20-50 years old, with men comprising 80% of cases. Unlike migraines, these headaches respond poorly to common painkillers and often require oxygen therapy or triptans for acute attacks. Chronic cases might need nerve blocks or verapamil for prevention.
Headaches triggered by effort or specific actions
Physical strain can trigger explosive headaches during:
- Coughing/sneezing
- Heavy lifting
- Intense workouts
- Sexual activity
Physical exertion increases intracranial pressure, which can trigger these headaches in susceptible individuals. Though usually benign, first-time exertion headaches require medical checks to rule out brain aneurysm or arterial issues. Most respond to beta-blockers, but sudden severe pain needs immediate evaluation, per a 2020 Springer study on primary headache disorders. Primary cough headaches specifically relate to activities increasing intra-abdominal pressure.
Thunderclap headache: a medical emergency
This “worst headache ever” peaks in under 60 seconds. Emergency protocols often involve immediate CT scans followed by lumbar puncture if initial results are inconclusive. Even if 60-80% prove benign after investigation, these headaches rule out life-threatening causes like brain hemorrhage or blood clots. Never self-diagnose – emergency evaluation matters most. Diagnostic criteria specifically require ruling out subarachnoid hemorrhage, which accounts for 1-3% of sudden headaches. While some patients develop reversible cerebral vasoconstriction syndrome (RCVS) with multiple thunderclap episodes over weeks, immediate imaging remains critical.
Hypnic headache: the alarm clock headache
Affecting adults over 50, these “alarm clock” headaches wake people at night (typically 1-3 AM). Unlike cluster headaches, they lack eye tearing or nasal congestion. Hypnic headaches are rare, affecting less than 1% of headache patients, and are often misdiagnosed as migraines. Treatments include caffeine before bed or lithium. Patients often experience multiple episodes per night, creating chronic sleep disruption. Though less painful than cluster headaches, their regular nighttime occurrence significantly disrupts rest patterns and daytime functioning.
When headaches are a symptom: understanding secondary headaches
Secondary headaches aren’t primary health issues. They act like alarm bells ringing from your body, signaling an underlying cause. These headaches often masquerade as common ailments – from medication dependence to neck problems – making proper diagnosis crucial. Let’s explore three key categories that frequently fly under the radar and why distinguishing them matters for effective treatment.
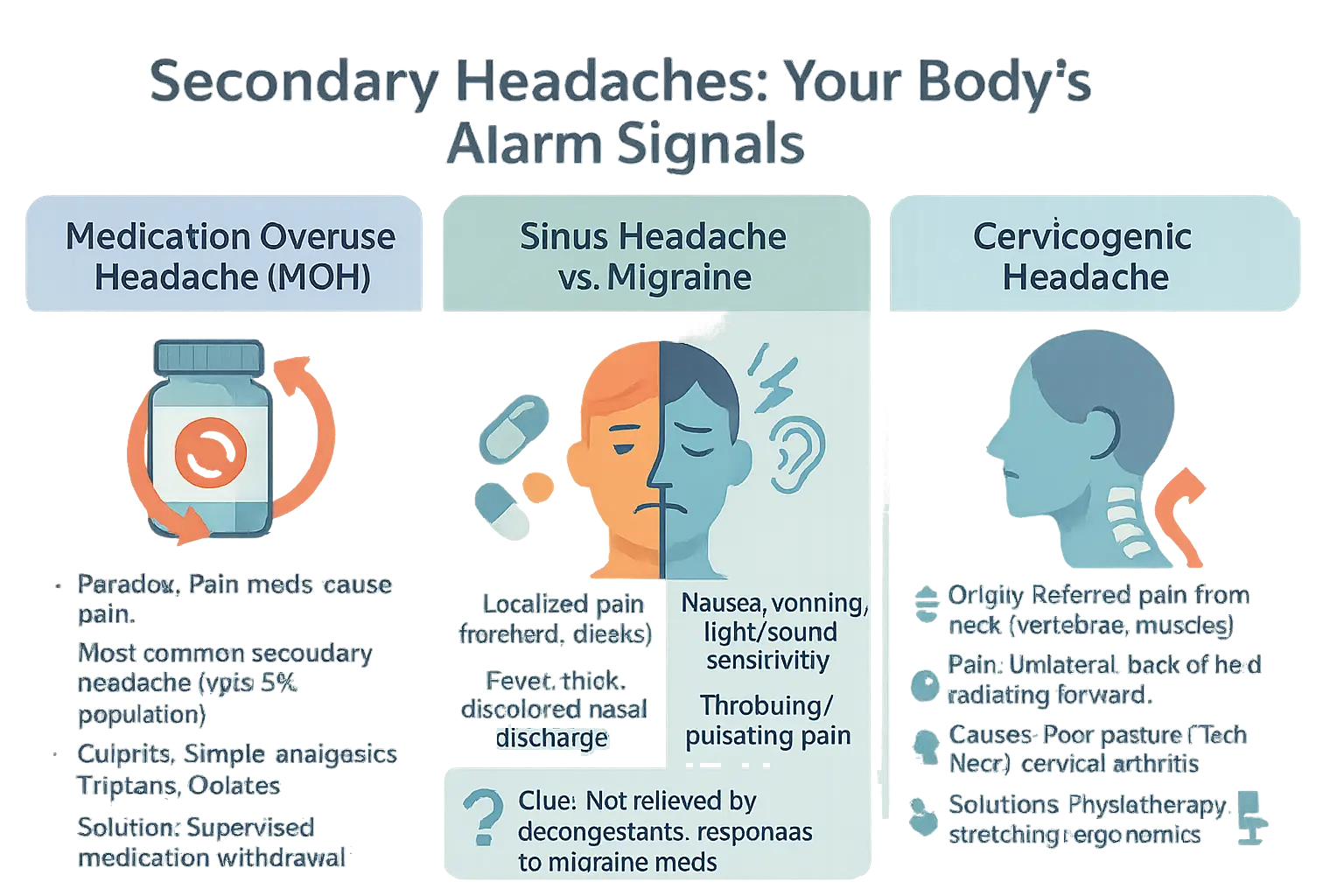
Medication overuse headache (MOH)
Imagine your painkillers becoming your problem. That’s the paradox of medication overuse headaches. When taken too frequently for migraines or tension headaches, these drugs create a vicious cycle of rebound pain. The World Health Organization estimates this affects up to 7% of certain populations, yet only 10% receive proper diagnosis. Consider this: for every 100 people with chronic headaches, 7 struggle with MOH while 90% remain undiagnosed.
Common culprits include:
- Simple analgesics like paracetamol (acetaminophen) used more than 15 days/month
- Triptans for migraine relief taken over 10 times/month
- Opioids and combination medications containing caffeine or barbiturates
Watch for morning headaches that won’t quit – a telltale sign. The solution? Medical supervision for gradual medication withdrawal. This isn’t about blame but breaking a cycle affecting 1 in 14 people. Beyond medication adjustments, keeping a headache diary helps track patterns and identify alternative treatments like cognitive behavioral therapy or acupuncture.
Sinus headache vs. migraine: learning to tell the difference
Think you’ve got sinus issues? Surprise – 90% of self-diagnosed sinus headaches are actually migraines. Real sinus headaches come with thick yellow discharge and fever from infections. Migraines masquerade as sinus problems with nasal symptoms, making diagnosis tricky. The confusion runs deep – even experts misdiagnose this 40% of the time.
- Sinus Headache: Thick, discolored nasal discharge and fever. Pain localized over infected sinuses. Typically follows cold symptoms or allergy flare-ups.
- Migraine: Nausea, light sensitivity, throbbing pain. Often mistaken for sinus issues. May include autonomic symptoms like tearing eyes or runny nose.
- Key Clue: If decongestants fail but migraine meds work, you’ve got migraines. Responds to triptans or NSAIDs.
Take the ID Migraine Questionnaire. Two “yes” answers mean 93% chance of migraines, not sinusitis. Three “yes” answers raise probability to 98%. This quick screening tool revolutionizes self-assessment for headache types.
Why does this matter? Misdiagnosis leads to inappropriate treatment – antibiotics for migraines or steroid injections for sinus issues. Proper identification saves time, money, and prevents unnecessary side effects from wrong medications.
Cervicogenic headache: when the pain comes from your neck
Your neck might be the culprit behind stubborn headaches. Cervicogenic headaches are referred pain from neck issues. Poor posture from device use creates “tech neck,” sending pain signals to your head. This connection explains why 22% of headache patients receive this diagnosis.
Common causes:
- Arthritic neck joints causing nerve irritation
- Muscle tension from poor posture creating trigger points
- Whiplash injuries altering cervical spine mechanics
Typical symptoms include one-sided pain radiating from neck to head, worsened by neck movements. Unlike migraines, it lacks light sensitivity or nausea. 72% of sufferers report improvement after physiotherapy. Treatment might involve manual therapy, posture correction, or ergonomic adjustments. Simple fixes like workstation setups or neck stretches work wonders for many patients.
Prevention includes posture awareness and device positioning at eye level. For persistent cases, nerve blocks or physical therapy address structural issues while dry needling targets muscle trigger points. Did you know? The International Headache Society’s ICHD-3 criteria help doctors distinguish cervicogenic headaches from other types through physical examination and imaging.
Headaches In Specific Populations: Children And Pregnancy
Headaches manifest differently across life stages, requiring tailored approaches for vulnerable populations. Children and pregnant individuals share commonalities in headache presentation but demand distinct management strategies due à unique physiological and safety considerations.
Understanding Headaches In Children And Adolescents
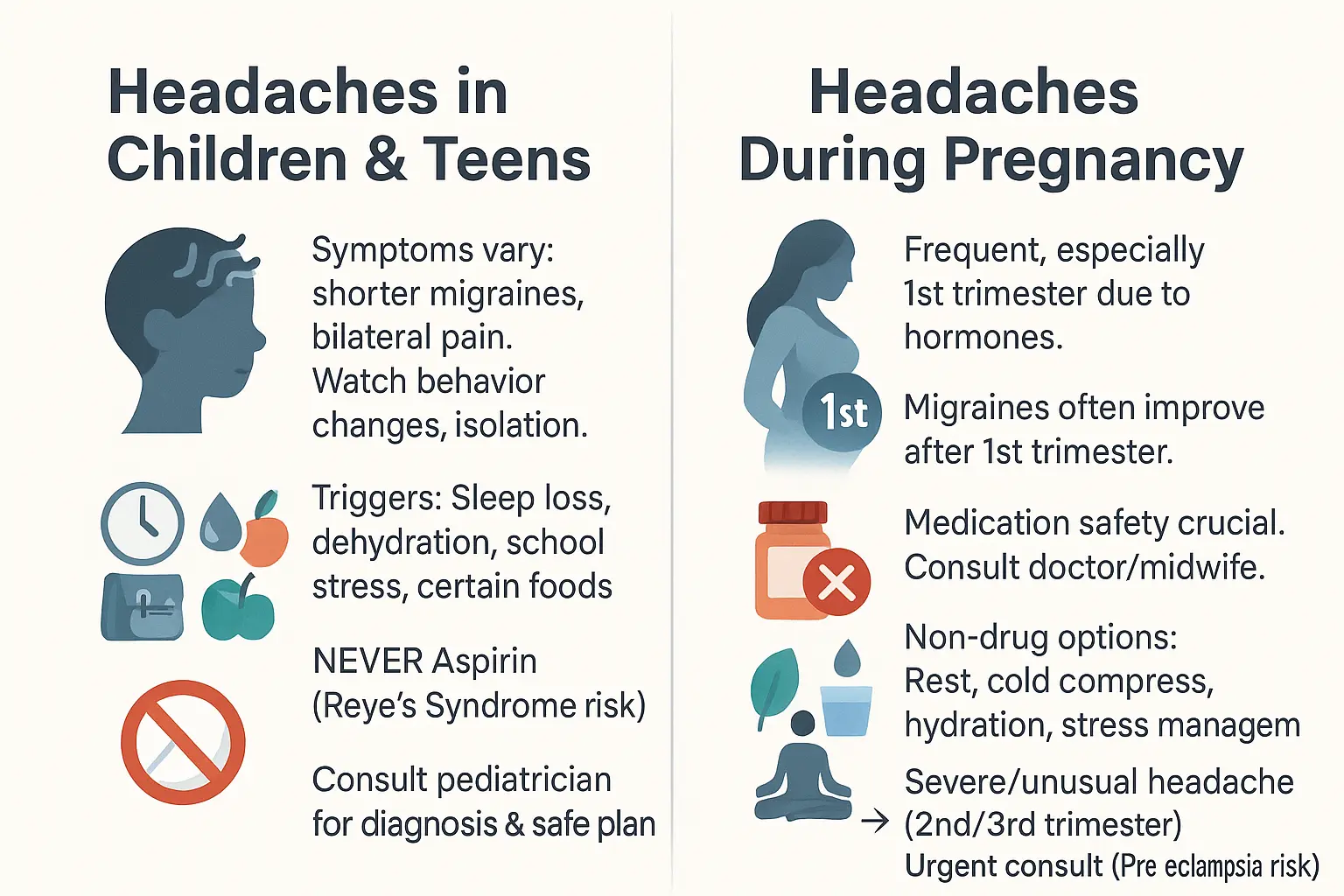
Headaches affect 60% of children by age 15, though symptoms differ from adults. Children might describe pain as “my head feels weird” or “it’s everywhere,” rather than localized pain. Key signs include sudden behavioral changes, avoiding play, or seeking dark quiet spaces. Migraine Quebec reports that pediatric migraines often last 2-72 hours with bilateral pain, sometimes accompanied by abdominal pain rather than typical adult symptoms.
Common triggers include:
- Sleep deprivation (25% of cases) – irregular schedules increase risk
- Dehydration (15% of clinic visits) – 2-3 daily water bottles prevent 1 in 5 cases
- School stress (30% of teens with chronic headaches) – exam periods worsen symptoms
- Dietary factors (tyramine in aged cheeses, nitrates in processed meats) – eliminate 2-4 week trial
Never administer aspirin to those under 18 due to Reye’s syndrome risks. This rare but fatal condition causes brain swelling and liver failure, often following viral infections treated with aspirin. French migraine association emphasizes immediate medical consultation for new-onset headaches in children, as 10% may indicate treatable issues like vision problems or sinus conditions.
Managing Headaches During Pregnancy
Over 80% of pregnant individuals experience headaches, most commonly tension-type or migraines. A large part of migraineurs report improvement after first trimester due to stabilized estrogen levels. Postpartum recurrence occurs in 40% within 3 months due to hormonal fluctuations.
Safe management strategies:
- Cold compresses (reduces inflammation in 70% of cases)
- Hydration (2.5L/day prevents 20% of pregnancy headaches)
- Gentle neck massage (improves blood flow in 60% of users)
- Modified prenatal yoga (reduces stress-related headaches by 40%)
Medication safety hierarchy during pregnancy:
| Medication | First Trimester | Second Trimester | Third Trimester |
|---|---|---|---|
| Paracetamol | Preferred choice | Preferred choice | Use cautiously |
| Sumatriptan | Limited use | Limited use | Avoid |
| NSAIDs | Short-term only | Short-term only | Contraindicated |
Seek immediate care for headaches with:
- Visual disturbances (5-8% risk of pre-eclampsia after 20 weeks)
- Severe pain after 28 weeks (1% risk of HELLP syndrome)
- Upper abdominal pain (30% of pre-eclampsia cases)
Pre-eclampsia develops in 5-8% of pregnancies after 20 weeks. Key signs include sudden weight gain (>2.3kg/week), facial swelling, and visual disturbances. Migraine France emphasizes urgent evaluation for any new-onset headache after 20 weeks gestation. Postpartum monitoring remains crucial as 25% of pre-eclampsia cases develop after delivery.
Red flags: when to see a doctor immediately
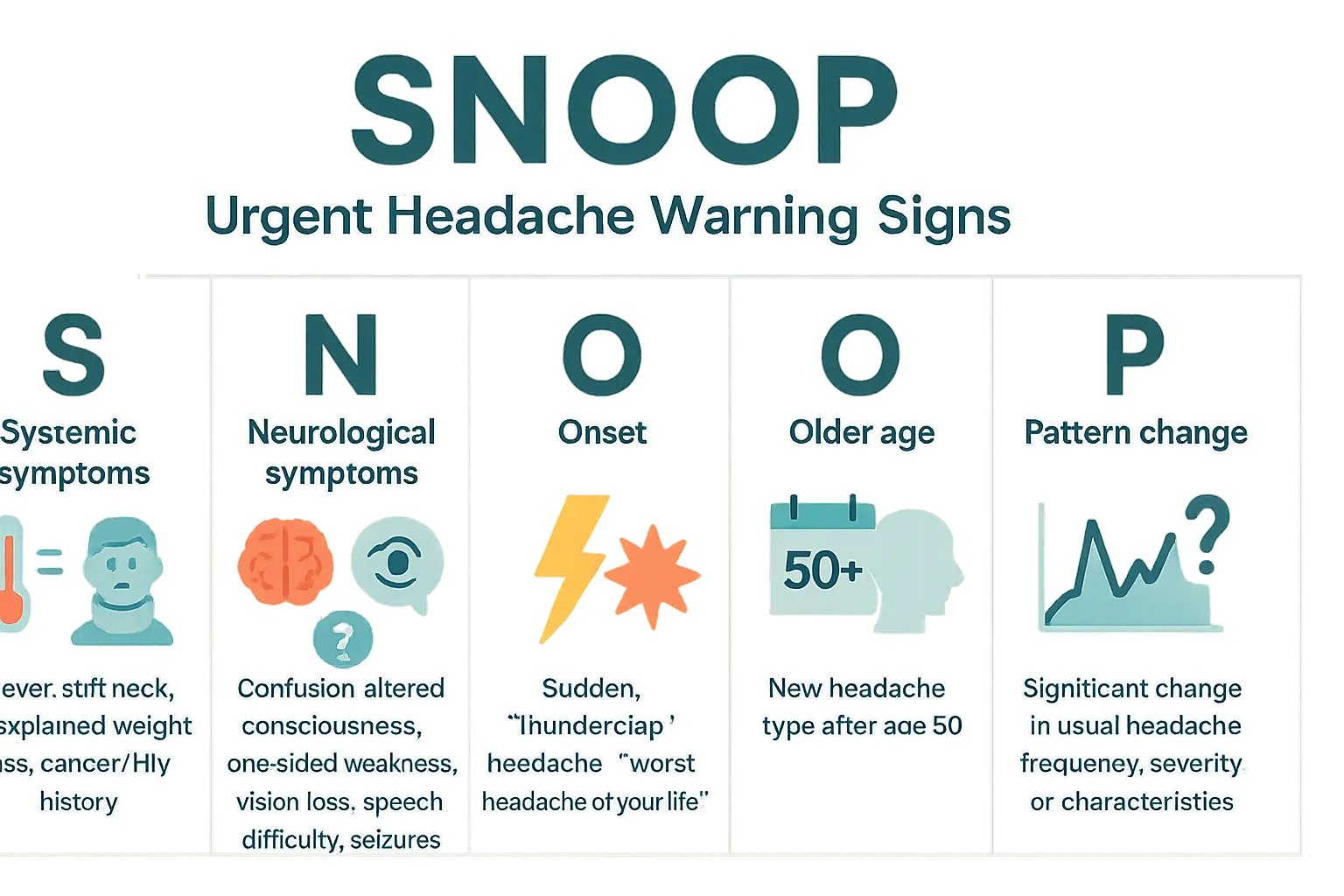
While most headaches resolve without intervention, urgent red flags require immediate medical attention. The SNNOOP10 criteria – a clinical tool used by physicians – helps identify dangerous secondary headaches. Understanding these warning signs can distinguish between ordinary discomfort and life-threatening conditions like aneurysms or meningitis.
- Systemic symptoms: Headaches paired with fever, stiff neck, or unexplained weight loss might indicate infections (like meningitis) or systemic diseases. For cancer survivors, new headaches could mean metastasis. HIV patients face elevated risks of opportunistic infections affecting the brain.
- Neurological symptoms: Sudden confusion, one-sided weakness, vision loss, speech difficulties, or seizures signal potential stroke, brain hemorrhage, or tumors. Facial drooping, arm numbness, or slurred speech demand emergency evaluation within 60 minutes.
- Onset: A “thunderclap headache” – the most severe headache of your life – that strikes suddenly and explosively requires urgent imaging. This symptom often precedes subarachnoid hemorrhage, with 50% mortality risk if untreated within 24 hours.
- Older age: New-onset headaches after age 50 raise concerns about giant cell arteritis (with vision loss risks) or slow-growing brain tumors. Blood tests like ESR/CRP become critical for diagnosis.
- Pattern change: Sudden escalation in frequency, intensity, or characteristics of existing headaches could signal evolving neurological issues like hydrocephalus or hypertension-related encephalopathy.
Additional urgent indicators include positional headaches worsening when lying down (possible brain tumor), exertion-triggered pain during coughing/sex (linked to aneurysms), or visual disturbances with eye redness (signaling acute glaucoma). According to Harvard experts, these symptoms warrant emergency evaluation regardless of headache history – even in young patients with clean medical records.
Never assume. If you experience any of these warning signs, call emergency services immediately. Prompt diagnosis can prevent permanent neurological damage, blindness, or save lives. Your health isn’t worth the wait – when in doubt, get checked out. Remember: “When a headache breaks your daily routine, it’s time to break the silence.”
How are other headaches diagnosed?
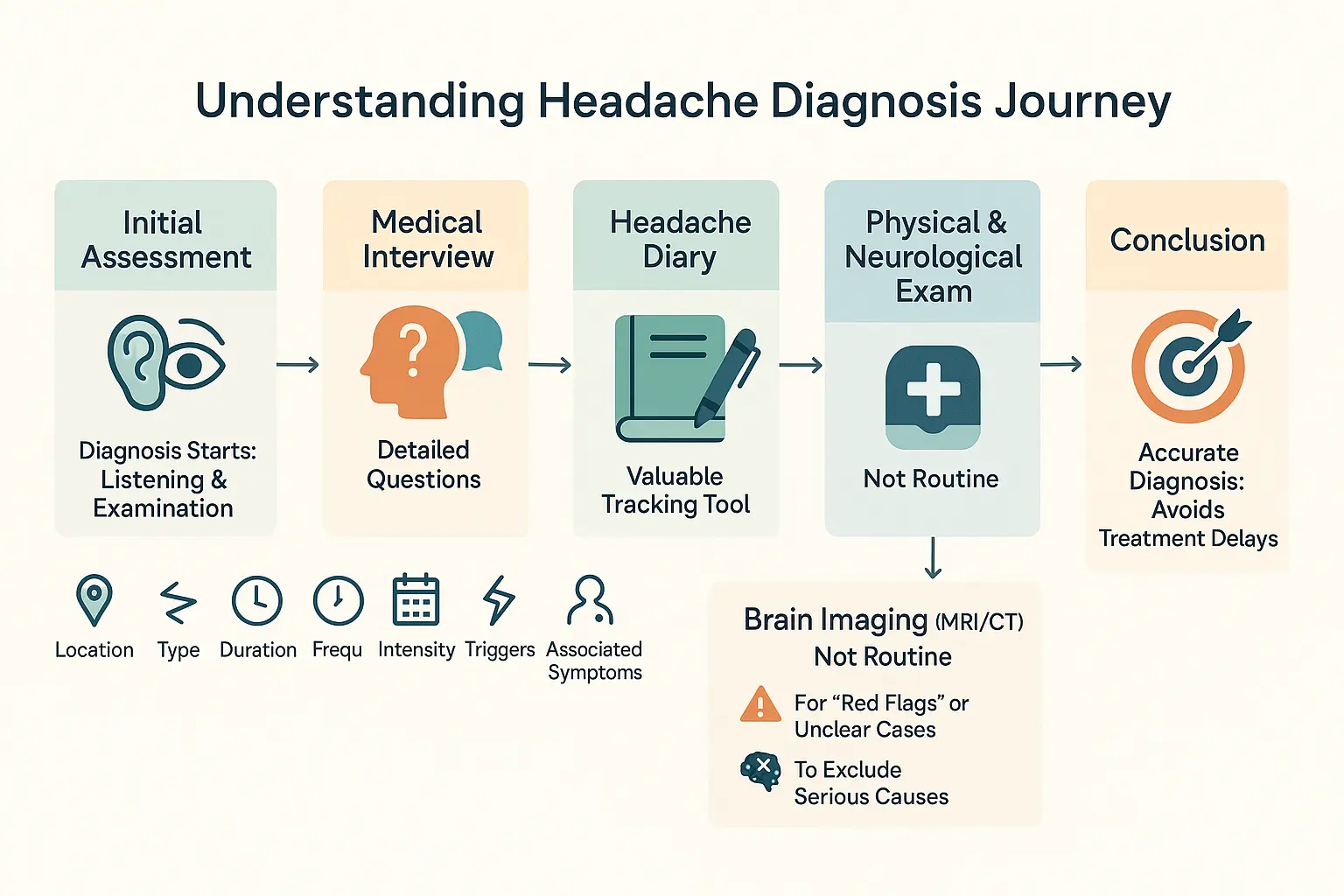
Medical Interview and Patient History
Doctors ask detailed questions about headache location, duration, intensity, onset (sudden vs gradual), and quality (pulsating, constant). They’ll explore triggers like activity, light, or specific foods (e.g., aged cheeses, processed meats), plus symptoms like nausea, light sensitivity, or visual disturbances (e.g., zigzag lines). Key details include frequency patterns, responses to over-the-counter medications, and connections to sleep issues, stress, or hormonal changes. This helps distinguish primary headaches (tension, cluster) from secondary causes requiring urgent care.
The Role of a Headache Diary
Recording dates, duration, pain intensity (1-10 scale), and triggers in a diary aids diagnosis. Headaches occurring 15+ days monthly might indicate chronic conditions needing specialist care. Tracking links lifestyle factors (stress, screen time, caffeine intake) to symptoms, guiding strategies like avoiding specific foods, improving sleep hygiene, or managing stress through mindfulness techniques.
Physical and Neurological Examination
Exams check red flags for secondary headaches: blood pressure (hypertension), neck stiffness (meningitis suspicion), or scalp tenderness (temporal arteritis). Neurological tests assess reflexes, muscle strength, coordination, and eye health. Unequal pupils or vision loss may signal neurological issues requiring urgent follow-up. Doctors also inspect nasal passages for infection signs and temporomandibular joints for inflammation that could mimic headache symptoms.
When Imaging Tests Are Necessary
Imaging (MRI/CT) isn’t routine but critical for red flags:
- Thunderclap headaches (subarachnoid hemorrhage risk)
- New headaches after age 50 (temporal arteritis or tumor concerns)
- Neurological deficits (weakness, double vision)
- Headaches worsening with straining or position changes (CSF leak suspicion)
These tests rule out life-threatening causes like aneurysms or brain lesions. Blood tests (inflammatory markers like ESR) may also be ordered. Always consult a specialist if headaches change in frequency, severity, or character – early diagnosis prevents complications like medication overuse or progressive neurological decline.
Navigating treatment and prevention for other headaches
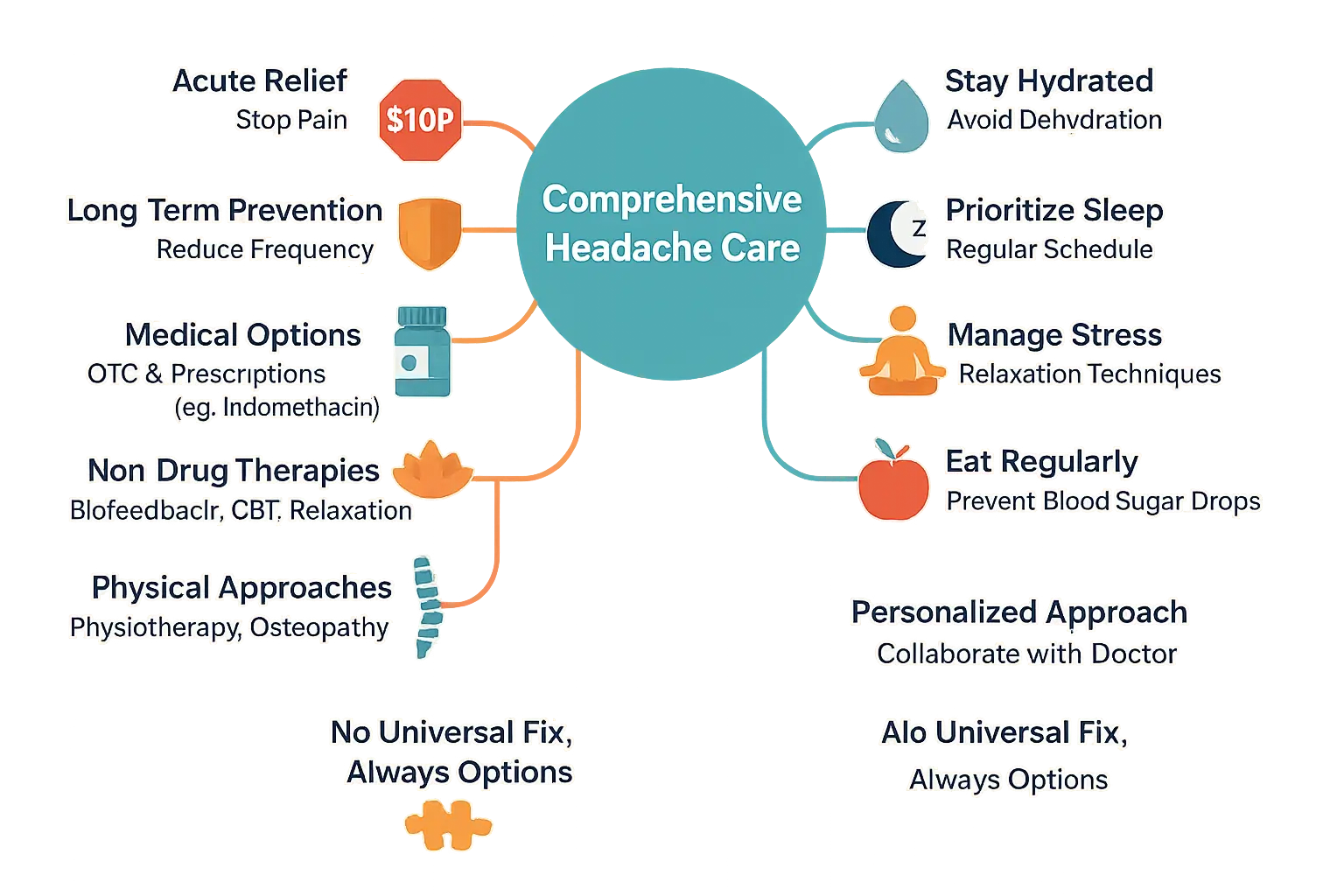
Managing headaches beyond migraines requires tailored strategies. Unlike migraines or tension headaches, rare primary headaches like exertion headaches or cough-induced headaches demand specific interventions. Treatment hinges on accurate diagnosis, separating acute therapies (to stop pain) from preventive approaches (to reduce frequency).
For exertion headaches or cough-induced headaches, Indomethacin remains a gold standard. The International Headache Society recommends doses between 25-200 mg/day, though exact regimens vary. For example, Chrono-Indocid (75mg) is often prescribed at 1-2 capsules daily. Always combine with stomach protectors due to gastrointestinal risks. Other options like acetazolamide or topiramate may apply in specific cases.
Non-pharmacological therapies offer complementary solutions. Biofeedback teaches pain control through physiological monitoring. Cognitive-behavioral therapy (CBT) addresses stress triggers. Physical therapies like osteopathy show promise for cervicogenic headaches, though evidence remains limited. Always consult a certified practitioner with proper credentials.
- Stay hydrated : Dehydration ranks among top headache triggers. Aim for 1.5-2 liters daily.
- Prioritize sleep : Irregular sleep patterns worsen headaches. Maintain consistent sleep-wake cycles.
- Manage stress : Techniques like meditation or gentle yoga can reduce tension-related episodes.
- Eat regularly : Skipping meals drops blood sugar, potentially triggering headaches. Small, frequent meals help.
Prevention thrives on lifestyle adjustments, but personalization matters. What works for cluster headaches might not help hypnic headaches. Always collaborate with healthcare providers to build a strategy matching your specific diagnosis. While no universal solution exists, combining medical and non-medical approaches often yields the best results.
 Headaches are as diverse as their causes, from migraines to cervicogenic pain. Understanding these differences empowers better management. Whether primary or secondary, each type requires tailored care. Remember, sudden or severe symptoms demand immediate attention. Always consult a healthcare provider for accurate diagnosis and personalized strategies to reclaim your well-being.
Headaches are as diverse as their causes, from migraines to cervicogenic pain. Understanding these differences empowers better management. Whether primary or secondary, each type requires tailored care. Remember, sudden or severe symptoms demand immediate attention. Always consult a healthcare provider for accurate diagnosis and personalized strategies to reclaim your well-being.
FAQ
What are the 7 types of headaches?
Headaches fall into two main categories: primary (the headache itself is the medical issue) and secondary (caused by an underlying condition). The most recognized types include migraines, tension-type headaches, cluster headaches, trigeminal autonomic cephalalgias (like SUNCT syndrome), and primary headaches triggered by specific actions (e.g., cough, exercise, or sexual activity). Secondary types, such as medication-overuse headaches (linked to excessive painkiller use) and cervicogenic headaches (stemming from neck issues), require addressing the root cause. According to the World Health Organization (WHO), over 300 types exist, but these seven are among the most studied and diagnosed.
When to worry about a headache while pregnant?
Headaches are common during pregnancy, especially in the first trimester, due to hormonal shifts. However, severe or sudden headaches in the second or third trimesters could signal preeclampsia—a condition marked by high blood pressure. Thunderclap headaches (extreme pain peaking in under a minute) are emergencies. Always consult your doctor before taking medications, as many aren’t safe during pregnancy. Non-drug approaches like hydration and rest are often recommended first.
Can shoulder pain cause headaches?
Yes. Shoulder and neck pain can lead to cervicogenic headaches, where pain originates from the cervical spine (e.g., poor posture, “tech neck,” or whiplash) and radiates to the head. These headaches are typically one-sided, starting at the back of the head and worsening with neck movements. Physical therapy and posture adjustments often help alleviate symptoms, as noted in studies on musculoskeletal causes of headaches.
What causes frequent headaches in children?
Common triggers in children include dehydration, irregular sleep, stress, and eye strain from screens. Kids might struggle to describe symptoms, so watch for behavioral changes like withdrawal or avoiding play. Avoid giving aspirin to children (linked to Reye’s syndrome) and consult a pediatrician for proper diagnosis. Keeping a headache diary can help identify patterns and guide safe treatment.
What does a pre-stroke headache feel like?
A pre-stroke or thunderclap headache strikes suddenly, reaching peak intensity in seconds. It’s often described as the “worst headache of your life” and may accompany neurological symptoms like vision loss or weakness. This is a medical emergency. Immediate imaging (like an MRI) is critical to rule out life-threatening causes like aneurysms or strokes, as highlighted in Harvard Health guidelines.
What is a red flag headache?
Red flags signal serious underlying issues. These include sudden onset (“thunderclap”), neurological symptoms (confusion, weakness), systemic signs (fever, weight loss), new headaches after age 50, or changes in a known headache pattern. The SNOOP criteria (Systemic symptoms, Neurologic deficits, Onset after 50, Pattern changes) help doctors prioritize urgent care, as noted in clinical studies.
How do you know if a headache is serious?
Use the SNOOP acronym: Systemic symptoms (fever, weight loss), Neurological deficits (vision loss, seizures), Onset (sudden, explosive), Older age (new headaches after 50), and Pattern changes (worsening or unusual symptoms). If any apply, seek emergency care immediately—these signs may indicate conditions like aneurysms or infections.
What are early signs of pregnancy?
Classic early signs include a missed period, fatigue, nausea, breast tenderness, and frequent urination. While headaches can occur due to hormonal shifts, they aren’t a definitive pregnancy indicator. Always confirm with a test and consult a healthcare provider for personalized guidance, especially if headaches are severe or persistent.
What are hormonal headaches?
These are migraines or headaches linked to hormone fluctuations, such as during menstruation, pregnancy, or menopause. Estrogen level changes often trigger them, explaining why many women experience migraines around their periods. Managing these headaches may involve hormonal therapies or lifestyle adjustments, as outlined in migraine research from institutions like the American Migraine Foundation.